►
Description
No description was provided for this meeting.
If this is YOUR meeting, an easy way to fix this is to add a description to your video, wherever mtngs.io found it (probably YouTube).
A
A
Stacy
I'm
not
sure
if
you're
talking,
but
you
are
muted
there.
I
am
okay,
so
you
know
technical
difficulties
again.
Sorry
about
that,
so
I
just
wanted
to
kind
of
talk
about
the
CDC
and
their
listing
for
organisms
that
are
great
concern
and
cre
has
made
that
list
and
is
considered
a
Threat
Level
urgent,
some
other
things
another
one.
A
There
we
go
so
you
know:
enterobacter
rallies
are
a
gram-negative
bacteria
that
you
are
commonly
aware
of.
We
see
it
all
the
time
in
people's
lab
results,
especially
in
the
elderly.
E
coli
is
one
of
them.
Klebsiella
pneumoniae,
enterobacter,
Cloquet,
serratia
marcessins.
These
are
all
gram,
negative
bacteria
that
can
be
cres.
A
And
carbop
enemies
are
carbopenums.
I
should
say
are
the
last
line,
antibiotics
that
are
used
to
treat
serious
multi-drug
resistant
infections
about
two
to
three
percent
of
bacterialities
are
associated
with
Healthcare
infections
that
are
resistant
to
carbopenums.
So
we're
not
talking
about
a
huge
amount
of
numbers,
but
it
is
creeping
up
there.
A
A
A
A
So
cra
is
transmitted
just
like
any
other
organism
can
be
direct
or
indirect
contact
with
someone
who's
infected
or
someone
who's
colonized
or
on
a
contaminated
surface,
but
in
healthcare.
It's
mostly
spread
by
people
passing
it
on
to
the
next
person,
usually
by
uncontaminated
hands
or
by
contaminated
shared
medical
equipment
and
in
some
instances,
sinks
and
drains
can
be
reservoirs
of
cre.
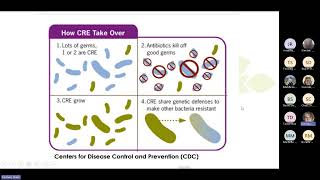
A
But
basically
you
have
this
bed
of
bacteria
and
you
have
very
few
cres
in
that
in
that
sample.
So
you
take
an
antibiotic
and
it
kills
off
all
the
organisms
that
are,
you
know
susceptible
to
that
antibiotic.
So
now
you
have
a
just
this
growth
of
cre
organisms
and
to
make
matters
worse.
Anything
that's
left
over
that
wasn't
or
was
susceptible
by
to
antibiotics
but
didn't
die.
A
A
A
A
A
It
means
that
the
cre
is
on
the
body,
but
it's
not
causing
illness
and
people
can
be
colonized
with
cre
for
months,
if
not
years,
and
that's
where
you
see
people
repeating
screenings
of
a
resident
to
see
if
they're
still
colonized,
so
they
can
take
them
off
of
special
precautions.
But
again
sometimes
you
can
see
people
who
who
are
colonized
for
years.
A
They
don't
have
any
signs
of
symptoms
of
illness
and
they're,
not
aware
for
the
most
part
that
they
are
colonized,
and
you
know,
those
who
are
colonized
are
at
risk
as
well
for
being
infected
with
Cris
series
or
an
opportunistic
bacteria.
And
so,
if
you
have
that
person
who's
got,
a
wound
has
lines
that
are
placed
urinary
tract.
You
know
or
urinary
catheters,
that
type
of
thing
they
are
at
risk.
A
So
I
just
wanted
to
show
you
some
data
that
I
came
up
with
looking
back
through
the
State
website.
I
only
went
back
to
2021
and
then
2023
to
date,
and
if
you
look
on
this
bottom
column
here,
Brown
is
this
year.
Green
is
last
year
in
2021
in
the
purple,
we're
really
seeing
some
static
numbers
as
far
as
those
infected
with
cre
or
colonized.
A
A
A
A
Good
news
is,
is
that
all
Laboratories
are
required
by
law
to
report
cre
positive
lab
results
and
those
reported
Labs
go
straight
to
the
the
state,
so
they
are
getting
those
reports,
but
if
you
have
a
new
cre
or
you
have
a
suspected
cre
outbreak
that
would
be.
You
know
two
or
more
in
your
facility
that
are
new.
A
So
so
you
know,
there's
no
harm
in
picking
up
the
phone
and
just
letting
people
know
at
the
state
or
even
with
us
that
you've
had
a
new
case
or
you've
had
several
new
cases
and
just
as
a
side
note
and
the
the
state
lab
does
have
the
capability
to
perform
CR
testing.
Not
all
Laboratories
have
that
capability.
A
So
there's
been
a
lot
of
debate
on
who's
eligible
for
screening
in
long-term
care
facilities
and
I.
Think
the
state
did
do
a
a
presentation,
probably
about
a
year
or
more
ago,
about
new
screening
guidelines
for
for
cre
and
some
of
the
others
like
carpa
and
crab,
but
but
for
cre
we
don't
advise
that
long-term
care
facilities
screen
all
new
emissions.
A
There's
really
no
data
to
support
that.
That's
probably
a
good
thing
to
do
at
this
time.
But
again
this
might
change,
but
you
should
screen
any
admission
that
has
had
an
overnight
stay
in
a
hospital
outside
the
United
States
in
the
past
six
months.
So
that's
really
the
the
one
one
where
you
have
to
to
do
that
screaming.
So.
A
A
Using
the
alcohol-based
hand,
sanitizer
is
just
fine
or
hand
washing
if
your
hands
are
visibly
soiled
before
and
after
resident
contact
and
you're
doing
this
anyways
with
all
of
your
residents
and
not
forgetting
to
do
hand.
Hygiene
for
your
resident
as
well
so
assisting
them
with
hand
hygiene
after
toileting
after
bathing
or
during
bathing
and
before
they
eat,
is
just
as
important
as
your
staff,
cleaning
their
hands,
cleaning
and
disinfecting
shared
medical
equipment
before
and
after
use.
A
If
you
have
somebody
who's
colonized,
and
you
know
that
they're
going
to
be
in
enhanced
precautions
for
a
good
while
if
you
can
dedicate
that
medical
equipment
to
that
person's
room,
that
would
probably
be
a
good
thing,
but
we
understand
that
that's
not
always
possible,
so
very
diligent,
cleaning
and
disaffecting
of
your
equipment
is.
Is
mandatory.
A
We're
going
to
talk
a
little
bit
more
about
enhanced
barrier
precautions
in
the
next
couple,
slides
and
then
participating
in
your
antimicrobial
stewardship
program.
I
know
that
this
is
something
that's
been
coming
up
in
CMS
as
well,
and
this
can
really
help
drive
your
compliance
with
not
using
unnecessary
antibiotics
or
limiting
the
use
of
antibiotics
in
your
facility.
A
A
So
enhanced
barrier
precautions
has
been
around
for
a
couple
years
and
it's
used
for
these.
You
know
multi-drug
resistant
organisms
of
concern
that
would
be
like
crab,
carpa
and
cres,
but
also
others
espls,
MRSA
and
the
like.
So
what
this
just
basically
means
is
that
you're
going
to
use
gown
and
gloves
when
staff
are
carrying
out
High
touch
activities,
so
if
they're
going
in
they're
doing
bathing,
they're
doing
toileting
they're
doing
dressing.
A
It's
recommended
that
for
any
Resident,
colonize
or
infected
with
an
mdro
have
enhanced
barrier
precautions,
but
it
also
can
be
used
for
residents
who
are
at
high
risk
for
acquire
acquiring
an
mdro
as
well.
Those
who
have
like
indwelling
lines
that
aren't
going
to
aren't
going
anywhere
just
a
chronic
line
or
people
who
have
wounds.
A
A
You're
only
doing
this,
if
you
feel
or
you
anticipate
that
you'll
be
doing
High
touch
activities
with
the
resident,
and
this
is
really
trying
to
balance
the
need
for
more
protection
with
with
your
staff
Staffing
and
trying
to
decrease
the
need
for
for
PPE
and
just
not
over
working
your
staff
with
trying
to
protect
the
rest
of
your
facility
and
just
like
in
standard
precautions.
Whenever
you
anticipate,
you
know
a
certain
risk
in
the
in
the
room.
If
you
anticipate
that
you
will
need
eye
protection
due
to
splashes,
especially
like
during
bathing.
A
It's
a
special
color
from
the
other
in
you
know,
transmission
based
precaution,
signs
and
it
just
really
kind
of
just
tells
people
what
they
have
to
do
as
far
as
entering
the
room.
So
they
they
list
out
quite
a
few
different
things
than
I
did
so
just
looking
at
those,
and
this
is
easily
obtained
on
the
internet
and
it's
free
for
use.
But
again
you
know
the
nice
things
about.
This
is
you're
only
going
to
use
your
gloves
and
gowns
during
High
contact
resident
care.
A
A
The
nice
thing
also
about
this
is
that
residents
can
participate
in
group
activities,
so
they
don't
have
that
sense
of
isolation
like
they
would
if
they
were
in
contact
precautions,
and
if
your
person
is
colonized
for
months
even
years.
This
enhanced
barrier
precautions
is
intended
to
be
used.
The
entire
length
of
the
residence
day.
A
A
You
know
it's
just
it's
just
kind
can
be
confusing,
and
especially
for
people
who
don't
go
in
and
out
of
the
rooms
more
frequently
than
than
some
other
staff
do
so
in
general.
Gowns
and
gloves
would
not
be
recommended
when
performing
transfers
in
common
areas
like
dining
or
activity
rooms,
and
that's
because
they
anticipate
that
that
contact
will
be
shorter
in
duration.
A
Is
it
perfect?
No,
but
this
does
give
the
resident
the
opportunity
to
join
activities
and
do
dining
room
activities
and
I.
You
know
just
really
decreasing
that
sense
of
isolation
outside
the
residence
room.
You
know
enhanced
precautions
should
be.
You
know
followed
when,
when
you're
performing
transfers
or
insisting
or
assisting
during
bathing
in
like
the
common
shower
rooms
or
if
they're
in
a
gym
and
your
physical
therapist
is
going
to
be
up
against
this
resident
for
a
prolonged.
A
A
And
here
are
some
resources,
basically
for
Series
in
particular,
the
CDC
I
put
that
in
there
cdphe
has
a
healthcare,
a
healthcare
acquired
infection
group,
a
team-
and
this
is
their
website.
This
is
their
phone
number
and
this
is
their
email
address.
I've
included
two
of
their
contacts,
their
epic
contacts.
So
if
you
have
any
questions
about
cre,
you
have
a
new
case
or
you
think
you
have
an
outbreak
of
cre.
You
want
to
use
this
email
address.
This
Hai
underscore
AR
at
state.co.us.
A
It
will
definitely
get
to
someone
who
is
monitoring
that
mailbox
and
they
will
return
your
phone
call.
If
you
have
any
questions
about
it
or
it's
still
not.
You
know
completely
sure
who
you
should
take
that
to
at
the
state.
I
put
my
own
email
address
in
here
in
my
office
phone
number.
If
you
have
questions
and
I
can
help
steer
you
in
the
right
Direction
and
get
the
right
people
from
the
state
to
to
return
your
phone
calls.
A
And
really
that's
all
I
have
on
cres
today,
just
to
plug
in
for
your
your
covid
booster.
Vaccines
are
coming.
You
know
available
here
in
the
next
week,
so
please
take
advantage.
Get
your
residents
vaccinated
flu
vaccine
is
available.
Your
RSV
vaccines
for
older
adults
are
available
and
just
to
plug
in
for
you
to
get
those
done
for
your
residence
and
your
staff,
not
RSV,
but
the
others
for
your
staff.