►
From YouTube: Commissioners' Briefing (January 5, 2021)
Description
Briefing of the Buncombe County Board of Commissioners for Jan. 5, 2021. No official actions take place at briefings. The purpose is for the board to hear upcoming news from staff and discuss future agenda items in an open, transparent manner.
A
A
B
B
A
B
Please
continue
thank
you,
so
cases
have
continued
to
climb
since
november.
What
you're
seeing
now
is
the
epi
curve
specific
to
us.
We've
currently
identified
995
total
cases
of
covet
19
since
pandemic
start
so
we're
about
a
day.
We
are
a
day
away
from
reaching
ten
thousand.
I
have
no
doubt
that
we'll
have
more
than
five
tomorrow,
and
so
we
saw
a
large
increase
post
thanksgiving
and
continue
to
see
those
cases
climb
post
christmas.
B
Trends
in
cases
have
not
changed
significantly
cases
site
gatherings
with
families
and
friends
both
in
the
home
and
outside
the
home,
as
in
their
investigations,
community
sites
and
work
sites.
Cluster
trends
have
not
changed
much
either
with
many
still
in
the
long-term
care
facilities.
Church
service,
medical
offices,
correctional
centers,
those
types
of
places
we
are
currently
seeing
about
134
new
cases
per
day
that
enter
our
public
health
workflow,
and
this
has
remained
stable
for
the
last
two
weeks.
Our
new
cases
per
100
000
per
week
after
a
week
of
stability,
has
begun
to
increase.
B
What
you're
seeing
now
is
the
statewide
percent
positivity
graph
and
that
percent
positivity
across
the
state
has
continued
to
increase
since
thanksgiving
with
our
current
state
rate,
at
16.5
percent
record
record
high
percent
positivity
across
the
state,
very
indicative
of
increased
community
spread
throughout
our
state
and
more
viral
spread,
and
just
to
give
you
the
local
perspective
locally.
The
percent
positivity
also
continues
to
rise.
The
percent
positivity
for
buncombe
county,
as
of
today,
is
11.4
percent
over
10
percent.
At
this
point,
that's
up
from
8.9.
B
Just
last
week
we
did
see
a
decrease
in
testing,
as
I
mentioned
that
many
people
going
so
you
had
less
people
getting
tested
and
only
going
if
they
really
were
feeling
symptomatic
and
really
thought
they
had
it.
So
you
start
to
see
some
of
that
being
affected,
but
overall,
it's
just
that.
There's
a
lot
of
community
spread
a
lot
of
viral
viral
spread
and
much
like
the
map
a
couple
slides
ago.
This
just
shows
you
what
the
percent
positivity
looks
like
across
our
state.
B
Hospitalizations
additionally,
the
hospitalization
statewide
continued
to
increase
seen
here.
The
daily
number
of
people
currently
hospitalized
with
covid
19
has
been
on
a
steady
incline
statewide,
since
just
after
thanksgiving
and
many
areas
of
the
state
started
to
see
that
right
before
thanksgiving
and
regionally,
we
don't
look
that
different.
We
are
seeing
the
same
trend.
Our
mission,
our
mission
hospital
hca
representative,
dr
hathaway,
is
here
with
us
today,
so
he'll
provide
more
of
that
information.
I
won't
spend
a
lot
of
time
on
that
today.
B
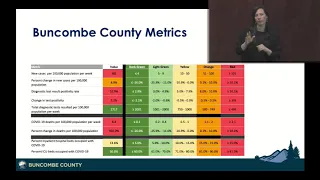
These
are
our
buncombe
county
metrics
that
we've
been
monitoring
over
time.
Many
of
our
current
metrics
that
we
monitor
remain
red
or
orange
at
this
time,
just
a
reminder
that
this
data
is
pulled
every
monday,
so
you're
actually
seeing
it
from
the
day
prior
just
so
that
we
have
some
consistency.
So
the
data
here
is
reflective
of
january
4th.
As
mentioned
earlier,
the
cases
per
100
000
per
week
has
increased
by
8.8
percent.
B
Our
percent
positivity
has
exceeded
10
percent,
and
now
we
saw
that
increase
by
2.2
percentage
points
from
last
week
and
testing,
as
I
mentioned
in
the
community,
actually
decreased.
It's
still
well
over
what
what
is
expected
or
what
is
recommended,
but
we
did
see
that
decrease
from
about
3
600
per
100
000
last
week
to
about
2
700.,
so
again
that
impact
of
the
holidays
is
likely
there
deaths
per
100.
000
population
saw
a
significant
increase
from
previous
week.
B
B
B
B
It
we're
getting
those
deeper
dives
and
those
more
detailed
documents
as
we
move
into
phases-
and
I
know
in
the
past,
our
board
members
have
been
interested
in
our
homeless
population
and
other
congregate
living
facilities
as
to
where
they
will
fall,
and
I
just
wanted
to
mention
that
currently,
if
they
meet
the
age
requirement
for
the
any
of
the
other
phases,
they
are
eligible
for
vaccine
there.
So
if
they
are
over
75,
they
can
get
vaccinated
in
1b.
If
they're
over
65
and
meet
that
criteria,
they
can
get
vaccinated
at
that
time.
B
Otherwise
they
will
be
that
over
65
will
be
in
the
early
stages
of
phase
two.
Otherwise,
if
they
meet
none
of
those
age
requirements,
they
will
be
in
the
later
phase
of
phase
two,
as
it
is
tentatively
planned
right
now,
and
I
just
wanted
to
share
that.
As
I
said,
dhhs
has
put
out
guidance
documents
that
provide
a
bit
of
a
deeper
dive
as
what
we're
calling
it
to
help
folks
understand
where
they
fall
in
these
vaccination
prioritizations.
B
I
won't
go
over
it
in
great
detail,
but
you
can
see
here.
This
is
that
1a
that
we've
been
focused
on
since
we
received
vaccine
on
december
21st
and
really
has
to
do
with
the
folks
who
are
caring
for
evaluating
testing,
doing
procedures
on
covid,
positive
or
caring
for
the
dead
of
that
and
then
the
deeper
dive
in
phase
1b
just
went
over
that
in
detail.
B
The
local
health
departments
are
expected
to
enter
this
phase
by
january
11th.
Some
of
them
may
be
ready
to
do
it
on
january
6..
They
can
do
they
can't
do
it
any
earlier
than
that
or
not
recommended
to
do
that,
and
the
expectation
is
january
11th
due
to
our
vaccine
supply,
we
will
begin
january
11th.
B
And
so
I
just
want
to
reiterate
that
opening
up
appointments
for
new
phases
also
is
heavily
dependent
on
how
much
vaccine
we
get.
So
we
might
get
an
estimate
of
how
much
vaccine
until
and
until
it
is
actually
at
the
health
department,
we're
being
very
cautious
as
to
open
up
appointments,
because
we
would
not
want
to
open
up
975
appointments
and
then
not
receive
that
amount
of
vaccine.
B
B
We
received
that
december
21st
and
we're
able
to
turn
that
around
in
24
hours
and
start
vaccinating
people
on
the
22nd,
so
just
an
amazing
feat
for
public
health
and
emergency
management
and
our
other
partners
and
then
december
30th.
We
received
975
and
began
using
that
on
this
week
january
4th
we
are
expected
to
receive
another
9.75.
A
B
Let
folks
know
that
I
recognize
for
folks
who
are
listening
to
us
and
streaming
live,
that
we
are
definitely
growing
weary.
I
understand
that.
I
know
people
are
tired
and
I'd
not
only
do
that.
I
understand
that,
but
that
your
public
health,
your
emergency,
your
emergency
management,
your
hospital
workers,
your
outpatient
providers,
all
understand
how
very
heavy
and
tiring
this
can
be.
B
But
I
want
to
urge
people
that
if
we
want
this
to
end,
we
still
have
to
be
very
diligent
about
some
other
things.
While
we
wait
for
vaccine
supply
to
increase,
and
that
means
stay
at
home
limit,
your
interactions
use
the
three
w's
even
with
family
and
friends.
When
you
know
them,
you
trust
them
still
use
the
3ws
and
get
your
vaccine.
When
it's
your
turn,
that
vaccine
is
an
incredible
gift
and
we're
all
very
excited
about
it.
D
Good
afternoon,
fletch
tove,
so
talk
about
our
rollout
operations,
our
fixed
sites,
the
actual
first
week
of
vaccine
distribution,
north
carolina
was
december.
14Th
during
that
distribution,
public
health
in
buncombe
county
did
not
receive
an
allotment.
Those
was
dedicated
specifically
to
hospital
systems.
D
Our
first
allotment
for
public
health
was
december
21st,
and
that
was
700
doses
of
moderna,
and
that
was
for
us
in
phase
one.
As
you
see
on
the
28th,
we
got
975
doses
of
pfizer,
and
then
we
did
just
receive
notification
during
this
meeting
since
stacy
stood
up
that
we
did
receive
this
week's
shipment
of
pfizer
and
up
another
9.75.
D
So
during
those
first
two
weeks
over
the
holidays,
we
administered
320
doses
a
week
and
then
finished
up
that
first
round
of
moderna.
Earlier
today
we
have
we
had
900
planned
for
this
week,
but
we're
looking
like
we're,
anticipating
some
bad
weather
on
thursday.
So
we
may
have
to
cancel
our
site
for
friday
for
safety
concerns,
but
should
still
reach
probably
about
600.
D
700
dispense
this
week
that
which
brings
us
into
next
week,
which
is
important
for
us,
because
we're
going
to
be
changing
the
location
of
our
vaccinations
to
increase
our
footprint,
which
would
take
us
up
to
a
capacity
to
do.
2000
vaccines
a
week
with
800
on
hand
we'll
be
able
to
push
through
our
current
supply
all
next
week,
so
really
we're
dependent
on
our
income
income
and
supply,
because
we
have
capacity
to
do
more
than
what
we
receive.
So
we
can
only
push
out
what
we
receive
and
we
have
to
from.
D
D
So
phase
one
a
as
stacy
went
over
was
long-term
care
facility
and
staff
and
patients
of
the
90
facilities
in
buncombe
county
that
are
not
covered
by
the
federal
pharmacy
program,
which
fall
that
charge
to
public
health.
We're
making
a
planning
assumption
that
there's
about
700
beds
accounted
for
and
we
for
we
don't.
We
know
not
all
those
beds
are
full,
so
we're
making
a
planning
assumption
of
about
500
doses,
we'll
have
to
go
to
those
long-term
care
facilities
and
that's
taken
from
that
weekly
allotment.
D
So
if
we
get
a
weekly
allotment
of
975,
those
vaccines
have
to
be
drawn
from
that
number.
We
don't
get
a
supplemental
dosage
and
then
we
also
we're
doing
first
responders
and
other
highest
risk
healthcare
providers,
which
we
had
a
planning
assumption
of
3
000.
so
during.
But
while
we
were
in
the
state
in
phase
1a,
our
total
allotment
was
1.
D
We
know
that
some
of
that
number
will
be
covered
by
phase
1a,
but
for
planning
assumptions
we're
making
the
number
40
000
with
a
current
allotment
of
1
000
doses
a
week
which
also
has
to
cover
the
remainder
of
phase
1a
and
the
state
has
allowed
us,
is
planning
for
phase
1b1
to
go
for
two
weeks.
So
you
can
tell
that
that
math
doesn't
add
up
if
we're
doing.
If
we're
getting
one
thousand
doses
a
week
to
vaccinate
a
population
of
forty
thousand
in
that
phase
is
two
weeks.
Clearly
we're
not
going
to
get
there.
D
D
phase.
One
b2
which
we'll
be
following
next
is
going
to
open
it
up
to
age,
50
and
plus.
You
know
healthcare
and
frontline
workers
of
that
age
group
and
we
we're
making
planning
assumptions
of
about
five
thousand.
But
we
really
it's
really
hard
to
drill
down
what
that
number
will
be.
But
we
are
hoping
in
the
coming
weeks
we'll
see
our
allotments
increase
greatly
from
the
975
or
700
we've
gotten
so
far.
D
We
also
for
those
long-term
care
facilities.
We
have
to
engage
in
mobile
vax
operations.
As
I
said,
there
are
90
long-term
care
facilities
not
covered
by
that
federal
pharmacy
program,
which
covers
you
for
public
health
to
cover
700
licensed
beds.
Again,
we
don't
think
they're
all
full.
We
think
for
planning
there's
about
500
patients
without
the
cover,
assuming
there
will
be
some
hesitancy
we've
already
seen
from
those
groups,
so
maybe
not
even
that
much,
but
that's
our
planning
goal
and
we'll
start
those
mobile
vaccines.
D
So
for
the
expansion
of
our
vaccine
operations,
north
carolina
dhhs
determines
the
timeline
for
these
phases
and
the
limiting
factor
on
our
throughput
is
the
state
allotment.
So
next
week
we'll
be
able
to
burn
through
all
the
vaccines
we
have
on
hand
and
we'll
be
dependent
on.
You
know
the
following
shipments
and
pushing
those
through
we're
relocating
our
our
fixed
site
to
av
tech
next
week,
which
will
increase
our
weekly
capacity
to
2000
at
our
fixed
sites.
D
D
I
just
also
wanted
to
discuss
that
public
health
is
being
extremely
supported
by
emergency
services
at
this
time.
So
when
we
talk
about
these
fixed
or
mobile
sites,
a
hundred
percent
of
the
logistics
support
for
those
sites
comes
from
emergency
services,
staff
and
personnel
and,
depending
on
the
site
about
25
or
50
of
the
manning
of
those
sites,
also
comes
from
emergency
services.
So
these
are
really
joint
efforts
between
public
health
and
emergency
services,
working
together
as
a
unified
team.
A
Have
one
quick
one
and
then
and
then
parker
parker,
that
I
mean
fletch
the
numbers
that
you
just
mentioned
of
the
975
a
week
is
that
only
what's
coming
to
buncombe
county
government
for
allocation?
Is
there
an
additional
much
larger
number,
that's
also
happening
in
parallel,
or
is
that
the
total
that's
our
community
is
receiving.
D
So
right
now
the
the
hospital
system
is
going
to
much
larger
supply
and
they
have
to
take
care
of
their
charge
as
well.
But
currently
there
are
no
no
vaccine
going
to
primary
care
providers.
There's
no
vaccine
going
to
pharmacies
we're
not
expecting
that
until
sometime
in
february,
so
right
now,
that's
the
allotment
for
the
county
and
it's
all
a
public
health
charge.
D
E
C
B
I
can
tell
you
sorry,
so
we
do
not
receive
a
formal
report
about
that
federal
program.
I'm
happy
to
inquire
more
about
it,
but
we
do
not
receive
any
type
of
report
about
what
is
being
sort
of
sent
out
in
that
and
other
than
that
they
are
getting
a
certain
allotment
of
the
state's
vaccine
into
that
program.
B
B
It
is
completely
parallel
like
it
is
completely
outside
of
what
local
governments
and
hospitals
are
doing
and
run
by
a
completely
different
entity,
and
so
I
will
just
say
caution
to
that
dashboard,
because
there
is
a
delay
in
that
information
too,
and
the
state
system,
which
is
called
cvms
while
has
potential
to
be
a
great
tool,
has
a
few
less
than
desirable
kinks
to
it
right
now
that
require
us
to
use
downtime
forms
and
those
types
of
things.
So
it
takes
a
little
while
for
that
to
get
uploaded
too.
C
Well,
ask
about
the
long-term
health
facility
situation,
just
because
I
I
want
to
know
that
it's
going
well,
and
so
I
guess,
give
us
a
high
level
explanation
of
how
that
works.
Is
it
walgreens
staff?
Is
it
the
staff
at
the
facility,
and
I
guess,
there's
all
kinds
of
news
reports
across
the
country
of
refrigeration
and
freezer
failures,
and
so
I'm
just.
I
just
want
to
know
that
it's
going
well
and
that
they're
adequately
staffed
and
have
what
they
need.
B
So
the
way
that
it's
supposed
to
work
is
that
that
allotment
goes
to
cvs
and
walgreens
that
then
distributes
distributes
it
to
their
teams
that
then
mobilize
and
do
that
vaccination
and,
as
I
said,
we
don't
get
too
much
more
information
about
what
that
looks
like
as
far
as
like
how
many
they've
done
but
I'll
be
happy
to
reach
out
and
see.
If
I
can
get
some
of
that
information
for
you
and
share
it
with
you,
but
I
do
not
have
any
of
that
right
now.
F
B
Now
that
we
know
that
shipment
is
here,
what
will
happen
is
so
we
already
have
the
steps
in
place,
so
we
were
being
very
cautious
not
to
open
those
schedules
just
yet.
So
what
we'll
do
after?
This
is
tell
folks
all
right
we're
ready
to
open
those
schedules.
We
have
a
phone
tree
ready
to
be
launched
and
then
the
public
release
that
will
be
launched,
hopefully
by
the
end
of
tomorrow,
with
instructions
on
how
to
get
an
appointment.
F
Thank
you
for
going
a
little
more
detail
there,
that's
great
a
couple,
more
quick
questions
again.
This
is
just
a
point
of
clarification.
It
sounds
like
the
largest
issue.
We're
encountering
right
now
is
sort
of
the
supply
chain,
side
of
it
and
that's
all
coming
through
the
state
and
that's
there's
no
other
way
to
get
the
vaccines,
except
through
the
state
and
that
problem's,
probably
originating
at
the
federal
level.
Correct.
B
B
F
I
know
you
all
are
in
the
deep
end
of
this
all
the
time,
so
these
questions
are
pretty
simple,
but
I
think
from
a
community
perspective,
these
are
the
kinds
of
questions
we're
starting
to
hear.
A
lot
of.
I
have
just
a
couple
more
looking
at
those
numbers,
especially
the
40
000
in
phase
2,
maybe
2
or
2b
1b1
1b.
F
I'm
sorry,
excuse
me
the
40
000,
that's
very
close
for
you
all
the
40,
000
and
and
then
thinking
about
the
timeline
of
all
of
2021
and
the
goal
of
probably
vaccinating
everyone
in
the
county
over
age
16,
if
not
more
by
the
end
of
the
year
at
some
point,
it'd
be
great
to
hear
y'all's
thoughts
on
capacity
needs
both
from
staffing
and
and
budgetary
perspective.
I
know
you're
probably
already
thinking
about
that,
but
it
would
be
great
to
start
that
conversation,
and
I
think
that
that
covers
my
questions
for
today.
B
So,
thank
you
thank
you,
and
I
just
want
to
say
that
commissioner
beech
before
that
you
had
mentioned
at
our
last
time
that
we
were
together
that
you
wanted
some
of
that
update
of
the
economic
impact
and
we're
working
on
that,
and
hopefully
we'll
have
that
for
you
soon.
So
we
knew
this
one
would
be
really
big.
So
probably
too
much
in
in
one
setting.
G
Before
you
go,
I'm
particularly
concerned
about
what's
going
on
with
the
african-american
community.
Oh
I'm
sorry,
I'm
sorry!
I'm
particularly
concerned
about
what's
going
on
in
the
african-american
community
and
especially
when
I
look
at
the
1b1
of
40
000,
I'm
in
that
group,
but
that
still
could
mean
I
would
get
a
vaccination
what
in
january
or
next
year,
you
know,
but
my
concern
is:
how
do
we
get
down
to
the
disadvantaged
people,
the
people
who
really
need
it
and
who,
I'm
afraid,
can
be
forgotten
during
this
process?.
B
That's
a
really
great
point:
I'm
glad
you
brought
it
up.
As
I
mentioned,
one
phase
1a
was
very
restrictive
to
support
that
health
care
system.
That
is
caring
for
the
coveted
positive
right,
so
that
that
was
extremely
prescriptive
as
to
how
that
was
going
to
come
out
and,
to
a
certain
degree,
even
1b1,
which
is
over
75
and
overs,
is
prescripted
and
it's
in
its
criteria
as
far
as
age,
but
as
part
of
our
planning.
We
do
talk
about
like
how
do
we
do?
How
do
we
do
this
in
a
more?
B
Populations
in
our
mind,
with
1a
that
that
didn't
necessarily
come
to
fruition
because
of
the
very
restrictive
and
prescriptive
nature
of
that
group.
It
is
definitely
at
the
forefront
of
what
we're
thinking
about
when
we
think
about
what
sites
are
we
going
to
do?
What
partners
are
we
going
to
engage
with
and
what
communications
we're
going
to
be
doing
as
far
as
town
halls
and
engaging
our
community
influencers
about
getting
that
information
out
and
also
you
know,
making
sure
that
folks
understand
that
we
are
limited
as
far
as
like
what
supply
we
get.
B
So
we
want
to.
We
want
to
vaccinate
people,
and
we
still
are
limited
by
the
number
that
we
receive,
and
so
you
know
we'll
be
reaching
out,
not
just
through
the
other
channels
that
we
did
even
through
coveted
testing
and
through
the
pandemic
of
how
to
get
that
information
out.
But
our
leaders
within
those
communities
to
help
us
get
that
word
out
and
help
folks
understand
how
important
the
vaccine
is,
and
so
very
with
one
a
that
that
you
know
that
just
wasn't
as
much
of
the
case
because
of
the
nature
of
that
group.
C
I've
got
one
more
thinking
about
you
touched
on
this
a
little
bit,
but
I
think
about
the
homeless,
and
I'm
also
thinking
about
you
know
some
of
our
partners
with
the
family
justice
center
that
work
in
the
domestic
violence
space
nonprofits.
That
sort
of
thing.
It
was
more
clear
to
me
in
the
previous
phasing
plan,
where
those
folks
fall.
So
I
guess
tell
me
if
you're
40
years
old
and
you
work
for
one
of
those
nonprofits
or
or
if
you're,
a
homeless
person
in
our
community,
where,
where
do
you
fit
in
this.
B
So
it
will,
some
of
it
is
depend
dependent
on
whatever
your
job
is
or
whatever
else
you're
doing,
and
so
I
don't
have
it
right
in
front
of
me
yeah,
but
for
one
b,
two
and
three
that's
gonna
be
direct
care
providers
and
they
do
right.
Now,
that's
that's
defined
as
direct
patient
care,
but
they
in
that
deeper
dive
really
go
down
into
that
about
what
that
might
mean.
Like
community
health
workers
right
some
care
managers.
C
H
You
I
want
to
follow
up
a
little
bit
on
commissioner
whiteside's
question.
I
appreciate
the
work
being
done
to
educate
folks
on
how
important
the
vaccine
is.
I
want
to
dig
a
little
deeper,
though
in
terms
of
working
with
those
community
partners.
Will
some
of
that
work
and,
as
I
talk
my
glasses
fog,
will
part
of
that
be
working
with
those
partners
to
actually
not
only
help
folks
schedule
their
appointments,
but
get
them
the
transportation,
the
child
care
the
things
that
they
need
to
leave
their
homes
to
get
the
vaccine?
B
B
B
Are
there
ways
for
us
to
do
this
so
that
you
know,
can
we
look
at
hybrids
of
walk-up
and
curbside
so
that
you
don't
have
to
be
necessarily
separated
within
a
space,
so
all
things
that
you
know
multi-faceted
things
that
we
are
thinking
through
and
as
we
get
to
those
bigger
phases,
engaging
not
only
our
internal
equity
work,
but
also
utilizing
those
community
partners
who
have
been
so
instrumental
in
that
too.
So
it's
still
so
much
to
be
determined
in
these
early
phases,
and
I
do
want
to
add
that
we.
I
A
I
have
one
other
kind
of
logistics,
question
or
timing
question.
So
it's
we
don't
know
at
this
time
what
the
ramp-up
schedule
is
going
to
be
like,
because
we
just
don't
know
how
many
are
going
to
be
arriving
into
buncombe
county.
So,
but
could
you
talk
us
through
when
what
you
can
share
about
when
we
do
expect
to
get
more
of
that
information?
A
Do
we
know
or
what,
when,
when,
might
we
get
greater
clarity
on
like
how
many
we're
going
to
get
in
january
february
march,
or
are
we
just
going
to
be
sort
of
learning
a
lot
all
along
the
way
and
like
maybe
in
the
end
of
this
month,
we're
still
not
going
to
know
what
we're
going
to
get
in
march?
It's
just
going
to
be
an
iterative
process,
or
at
some
point
will
the
scale
up
of
this
vaccine
distribution
process
become
a
little
more
clear.
B
B
I
D
A
So
if
we,
if
we
were
doing
2
000
a
month,
I
mean
2000
a
week
which
is
around,
let's
say,
9
000
a
month.
That's
just
what
the
county
itself
is
administering
is
the
expectation
that
that's
just
a
relatively
modest
percentage
of
the
total
distribution
in
the
community,
and
I
mean,
of
course,
we're
all
just
really
eager
to
understand,
like
by
january
march
april,
what
percentage
of
our
community
is
going
to
have
received
a
vaccine?
Well.
D
We
know
in
february
we're
expecting
for
primary
care
providers
and
pharmacies
to
receive
allotments
to
start
doing
their
their
own
coverage
for
their
charges.
But
currently
all
that
burden
is
on
public
health,
and
you
know
the
hospital
has
resources
as
well
they'll
be
able
to
expand
to
the
community.
C
B
And
so
the
expectation
is
that
by
february
those
other
providers
like
fqhc's
community
health
centers
other
community
medical
staff,
would
be
completely
enrolled
as
providers
and
be
able
to
launch
as
providers
it's
still
unknown
if
they
will
be
able
to
get
their
any
vaccine
allotments.
At
that
time.
A
B
A
D
Do
want
to
take
one
moment
to
ask
patients
from
the
community.
I
know
for
phase
1b1
when
we
have
tens
of
thousands
of
people
who
may
be
looking
to
reserve
a
schedule
for
next
week
and
we
may
only
have
a
thousand
spots
to
open
and
then
the
following
week.
A
thousand
again,
we
have
you
know,
maybe
thirty
thousand
people
trying
to
buy
for
the
spots
just
patience
and
for
you
I
expect
you
guys,
will
see
many
emails
of
people
upset
at
that
process,
but
understanding
the
constraints
we
have.
A
J
How
the
way?
Oh,
I
appreciate
it.
Thank
you
chairman
newman.
I
was
going
to
start
out
with
an
update
on
the
hospital,
but
I
think
with
all
the
conversation
about
the
vaccine,
it's
more
apropos
to
just
continue
that
conversation.
I
I
sense
the
frustration
in
each
of
your
questions
and
the
exasperation
behind
your
masks.
I
think
the
maths
are
probably
a
good
thing
for
you
right
now.
J
It's
been
a
very
trying
and
challenging
process
to
to
comment
and
elaborate
on
a
few
of
the
things
that
both
stacey
and
fletch
have
commented
on
already
we
number
one
that
the
county
is
or
the
state
is
allocating
by
county.
So
when
they
look
at
the
doses
that
we've
received,
they
look
at
the
doses
that
have
gone
to
mission
health
system.
They
look
at
the
doses
that
have
gone
right
now
to
the
health
department,
and
so
that's
a
that's
an
aggregate
number
that
they
look
for
future
allocations.
J
The
dashboard
that
you're,
looking
at
at
the
state
level,
the
documents
how
much
vaccine
has
been
given
is
wildly
inaccurate
right
now,
because,
as
stacy
saunders
said,
that
there's
delay
in
the
data
and
the
state
vaccination
registration
system
called
cvms
has
been
really
fraught
with
major
problems
and
we
administered
our
initial
series
of
doses
completely
on
downtime
forms
were
unable
to
administer
any
doses
within
the
system.
So
I
I
I
have
confidence
that
it
will
come
up.
J
It's
new
they're
working
on
it
hard,
but
right
now
don't
don't
draw
any
conclusions
based
on
that
data.
At
this
point
we
have
received
almost
10
times
as
much
vaccine
as
the
as
the
county
has,
which
is
good
news
and
bad
news.
We've
received
we've
administered,
3,
700
doses,
to
our
1a
health
care
providers,
which
is
good
news.
J
J
So
if
you
do
just
quick
back
the
napkin
math,
if
we
get
a
75
uptake
rate,
we
should
have
enough
to
cover
all
those
folks,
I'm
not
sure
we'll
have
it
that
high.
It
remains
to
be
seen
what
people
are
going
to
do.
I
think
a
lot
of
people
are
apprehensive
and
waiting
to
get
it.
We
fully
plan
to
expand
our
vaccination
within
the
community
to
include
when
we
can,
as
we
move
through
our
own
internal
tears.
J
You
know
office,
practitioners
and
dentists
and
other
people
in
the
community,
first
responders,
etc.
When
we
can
do
that,
how
I'm
going
to
do
that?
How
I'm
going
to
get
it
scheduled?
What
it's
going
to
look
like
when
it's
going
to
happen?
Those
are
all
if
you
have
answers
for
me.
I
would
welcome
your
input
on
that.
The
cvms
system
has
been
a
challenge.
Our
scheduling
system
internally
has
been
a
challenge.
J
It's
not
as
simple
as
as
a
massive
flu
vaccination
campaign
where
we
can
simply
go
out
and
stick
needles
in
arms
and
not
worry
about
it.
We
have
to
document
the
dose
make
sure
we
know
what
lot
they
got,
because
we
have
to
be
sure
if
there's
any
problems
with
this
vaccine,
that
we
can
track
the
people,
we
have
to
make
sure
that
we
know
where
they
had
the
dose
administered.
The
the
logistics
are
complicated.
So
it's
just
to
echo
the
the
what
stace
and
flesh
said
about
begging
patients
of
the
community.
J
That
being
said,
we're
making
great
progress
when,
if
we
have
extra
doses
of
vaccine
I
I
don't
want
it
sitting
on
the
shelf
right
now
and
if
we
think
we
can
get
supply
later,
we'll
do
what
we
can
within
reason.
We
meet,
we
talk
stacey
and
I
talk
every
week
or
more
often
and
we'll
do
what
we
can
to
get
the
vaccine
where
it
needs
to
go
to
get
in
people's
arms.
It's
really
important
that
that
happens
soon.
J
If
we
look
at
275
000
people
in
buncombe
county-
and
we
look
at
you-
know,
250
doses
a
day-
that's
only
90
000
doses
in
in
a
year,
so
this
is
going
to
take
time
for
us
to
ramp
up
it's
incumbent
on
us
who
are
charged
with
this
responsibility
to
work
collaboratively
across
silos
with
one
another
to
really
build
the
infrastructure.
To
make
this
happen,
they
can't
do
it
alone.
We
can't
do
it
alone.
J
This
is
going
to
take
everybody
in
the
community
to
make
this
happen,
and
so
we're
working
actively
with
the
team
to
to
to
try
to
do
that.
I
wish
I
could
give
you
more
details
about
you
know
what
the
slope
of
the
curve
looks
like
when
we're
going
to
hit
these
certain
landmarks,
it's
critically
dependent
on
lots
of
other
issues,
and
I
think
you
heard
just
before
this
meeting,
that
the
governor
has
talked
about
bringing
the
national
guard
in
to
help
with
some
of
this
it
sounds
like
you
know.
J
The
white
horse
is
on
the
way.
That's
every
little
bit
is
going
to
help,
but
that's
just
the
beginning
phase.
We
need
permanent
places,
long-term
solutions
and
a
long-term
strategy
across
multiple
organizations
to
get
this
done
so
we'll
work
on
that
any
specific
questions
for
us
about
what
we're
doing
at
the
hospital.
At
this
point
or
anything,
I
can
further
elaborate
on.
J
It's
it's
a
question
that
we're
actively
addressing
right.
Now
we
there
this
hospital,
the
state,
has
deployed
the
vaccines
in
two
different
ways.
One
is
a
closed
pod
and
one
is
an
open
pod
and
we
applied
for
closed
pod
distribution,
which
meant
our
health
care
facilities
and
the
workers
and
other
people
affiliated
with
it.
J
We
are
planning
to
step
outside
those
bounds,
a
little
bit
to
make
sure
that
we
address
all
the
other
folks,
but
I
don't
want
to
make
a
global
commitment
at
this
point
in
time
until
I
know
what
we
can
handle
without
massively
disrupting
our
other
operations,
which
I'm
going
to
talk
in
a
moment
which
is
caring
for
all
these
covet
patients,
which
are
you
know,
washing
up
on
our
shores
in
droves.
So
we're
really.
We
got
a
double
double
responsibility
here.
We
will
do
what
we
can.
J
We
want
to
help
we'll
do
we'll
cooperate
and
participate
in
in
any
way
that
we
can,
but
I
can't
make
detailed
promises
about
what
that'll
look
like
right
now,
so
that
gets
to
the
next
question.
I
appreciate
you
asking
that
the
the
next
issue
is
what's
happening
in
the
hospital
system.
I
think
people
are
aware
that
we
have
seen
more
patients,
not
just
at
mission
hospital,
but
at
all
the
hca
facilities,
and
I
have
daily
calls
with
the
other
cmos
in
the
region-
part
e.
J
As
an
example,
it
was
in
the
30
to
40
range.
They
used
to
have
less
than
10
patients.
Haywood
county
was
over
25.
Today,
haywood
regional
harris
is
above
20,
advent
was
pushing
20,
and
these
are
all
facilities
in
the
region
which
had
less
than
a
half
a
dozen
patients
for
most
of
last
year.
In
november
of
this
past
year,
we
had
40
patients
in
our
hospital,
and
today
we
are
at
over
130
at
missions.
So
we've
tripled
more
than
tripled
our
numbers
in
two
months.
J
We
knew
that
would
happen
that
it
would
rise
as
the
result
of
the
thanksgiving
holiday.
What
surprised
me
was
that
the
rise
occurred
even
before
the
holiday
began,
and
it's
you
saw
the
numbers
that
stacy
showed
the
epicurve
for
buncombe
county,
exactly
the
same
shape
of
the
curve
for
our
hospitalizations,
just
a
different
y-axis,
of
course.
So
it
is
hugely
concerning
to
us
that
the
numbers
continue
to
rise
and
we,
as
stacy
has-
and
I
have
in
other
forms-
have
repeatedly
pleaded.
J
We're
often
questioned
about
what
our
capacity
issues
are
at
the
hospital
we
have
a
complicated,
I
shouldn't
say,
complicated,
a
sophisticated
and
complex
set
of
metrics
that
we
look
at
to
to
determine
how
we're
doing
percent
of
patients
in
our
icus
who
are
covet.
Related
percent
of
patients
on
ventilators
percent
of
ventilators
used
ppe
on
hand,
etcetera.
It's
a
very
it's
a
detailed
spreadsheet,
which
I
brought
with
me
in
case.
There
are
any
specific
questions.
J
I
I
don't
think
the
details
matter
for
the
purpose
of
this
conversation,
except
to
say
that
we
look
at
this
every
day,
trying
to
determine
how
our
capacity
needs
are
being
met.
We
went
on
a
big
campaign
to
hire
additional
nursing
staff.
Our
biggest
concern
is
not
beds
or
ppe
right
now.
It's
nursing
staff,
that's
a
you
know.
Human
capital
is
a
finite
resource
and
a
valuable
one
that
we
need
to
really
take
care
of,
and
they're
they're.
Getting
worked
very,
very
hard
right
now.
J
We've
had
to
stretch
our
ratios
as
have
the
other
hospitals
in
the
community
as
everybody
across
the
country
you're.
Seeing
that
nursing
shortage
is
real
and
we're
doing
everything
we
can
to
meet
that
need
right
now,
we're
okay,
we're
we're
it's
not
where
we
want
it
to
be,
but
we're
I'll
use
the
okay
in
quotation
marks
and
and
and
we're
watching
that
closely.
We're
often
asked
about
procedures.
J
If
you
remember
earlier
in
the
year,
there
was
a
move
to
curtail
what
we
called
non-essential
and
I
always
struggle
to
find
the
right
word,
because
the
procedures
that
were
stopped
were
essential
to
the
people
who
are
needing
them,
and
we
have
to
be
mindful
that
when
we
term
something
elective,
it
only
means
that
it's
not
a
hyper-emergency.
But
if,
if
you
had
a
breast
mass
and
you
needed
it
removed,
that
would
not
be
considered
elective
in
most
people's
eyes,
but
in
many
ways
it
was
previously.
J
We
look
at
the
procedures
that
we
think
might
occupy
an
inpatient
bed
afterwards
and
and
are
watching
that
closely
and
if
and
when
we
get
to
a
point
where
we're
at
capacity
pressure
points
we'll
we'll
focus
on
those
procedures.
First,
stopping
surgeries
and
procedures
in
the
outpatient
setting
you
know
in
the
ambulatory
surgery
setting
doesn't
do
anything
to
free
up
resources
and
it
just
delays
care.
So
I
raise
that
to
you
all,
because
I
appreciate
your
concern
from
prior
conversations.
J
J
We
are
I
used
to
talk
about.
You
know
the
the
lapping
at
our
shores.
You
know
kind
of
euphemistically,
because
we
were
isolated
geographically
here
and-
and
you
know,
when
we
hit
40,
I
thought
50.
How
are
we
going
to
handle
50?
You
know
we've
learned
how
to
handle
it,
but
we
are
deep
in
the
surge
right
now
and
it's
going
to
get
worse.
The
numbers
are
going
to
go
up
higher.
We
will
have
somewhere
between
150
and
200
patients
in
the
hospital
we're
preparing
for
that.
J
I
raise
that
not
to
I
raise
that
for
two
reasons,
one
to
provide
some
level
of
reassurance
that
we're
planning
for
it
and
also
to
to
really
tell
the
community
that
this
is
real
and
we
need
your
help.
You
know
the
the
solution
is
not
stopping
elective
procedures.
The
solution
is
not
coming
to
the
hospital
in
the
first
place
with
coveton,
so
we
really
really
need
everyone's
help
in
that
regard.
F
F
J
Yeah
I've
thought
about
that
question
a
lot
it
was
asked
previously.
We
we
made
a
decision,
so
our
our
acceptance
of
transfers
is
is
a
very
complicated
process.
It's
dependent
on
bed
availability
and
it's
dependent
on
skill
set
to
take
care
of
the
patients
and
it's
dependent
upon
recognizing
that
we
are.
J
We
see
the
18
county
region
as
our
priority
and
our
responsibility,
and
so
there
have
been
times
when
we've,
you
know,
stopped
transfers
from
out
of
state
for
inpatient
vets,
because
we
want
to
be
sure
that
we've
had
that
capacity.
You
know
we
we
will
we
it's
a.
You
know
we're
in
medicine
because
we're
humanitarians
and
we
care
about
people.
We
don't
want
to
see
anyone
in
trouble,
but
we
will
have
lots
of
conversations
about
how
we
globally
manage
that
across
the
state.
J
A
Dr
hathaway,
when
you,
when
you
say
you
know,
we've
gone
from
40
to
130,
of
course,
that's
very
troubling,
and
it's
going
to
keep
growing
realistically,
we
could
have
150
to
200
patients
in
the
hospital
is
and,
like
you
said,
you
have
some.
You
have
some
levers
right.
There
are
things
you
don't
want
to
defer,
but
if
we
absolutely
had
to
you,
you
could
do
those
things
trying
to
bring
in
new
staff.
A
Is
that
what
do
you
see
as
sort
of
where
you
know
the
capacity
of
the
the
hospital
when
you
sort
of
start
running
out
of
options?
And
it
you
know
the
scenario
where
we
talk
about
facilities
being
overwhelmed
like
we
get
there
and
there's
there's
really
not
other
good,
short-term
solutions
to
it
like
what.
J
J
I,
with
you
know
again:
it's
not
there's
not
a
single
point,
but
I
think
conceptually
when
we
get
to
a
point
where
we
can't
routinely
accept
transfers
from
the
region,
for
whatever
is
bothering
people
because
remember
the
strokes
and
heart
attacks
and
kidney
failure
and
everything
else
is
going
on.
So
when
we
get
to
a
point
where
that
routinely
becomes
a
problem,
then
we
need
to
look
at
how
we
create
additional
capacity.
J
That's
probably
one
of
the
things
that
worries
me
the
most,
because
we
have
we're
not
just
a
covet
hospital,
we're
a
we're.
You
know
a
tertiary
and
coronary
care
hospital
where
we
care
for
everybody
in
the
region.
We
recognize
that
responsibility,
so
that
would
be
one
if
the
stashing
staffing
ratios
to
accomplish
the
care
are
just
untenable.
J
That
would
be
another
one,
and
I
recognize
that
you
know
anything.
That's
not.
What
is
normal
is
untenable
for
those
who
are
providing
the
care
of
those
patients,
and
it's
important
that
I
I
take
a
pause
here
just
to
thank
the
the
people
who
work
in
our
facilities,
because
you
know
we
we've
you've
heard
it
since
the
dawn
of
the
pandemic,
that
they're
the
heroes,
but
they
that
now
they
are
really
her
doing
the
heroic
work
here,
and
I
just
want
to
recognize
that
we
acknowledge
that.
A
And-
and
I
realize
there
are
these
different
ways
that
you
can
help
manage
this,
and
these
numbers
don't
stay
fixed
in
time
because
of
different
things.
That
can
be
done,
but
I
mean
is
it
possible
for
the
hospital
to
share
with
us?
You
know
community,
you
need
to
know
like
we
have
this
much
more
capacity,
but
you
know
if
we
go
beyond
this
point.
It's
we're
really
like
it's.
It's
going
to
be
really
bad
for
the
folks
who
are
getting
sick
from
covet
or
something
else
and
the
other.
A
The
other
question
I
would
ask
would
be
what
are
those
ratios
which,
if
we
go
beyond
them,
really
are
considered?
You
know
that's
unacceptable
and
are
those
things
that
you
that
can
because
we
all
anticipate
the
next
couple
of
months
are
going
to
be
really
tough
and
I
guess
just
to
the
extent
the
community
can
really
understand
those
dynamics,
whether.
J
It's
good
news
or
bad
news.
I
think
as
well
as
examples
without
getting
too
much
into
the
specifics.
You
know
if
we
have
a
nursing
unit,
which
typically
one
nurse
cares
for
four
or
five
patients,
and
because
of
sick
staff
members
or
extra
patients
they're
up
to
one
to
six
or
one
to
seven.
While
that
may
work
for
a
short
time,
that's
not
a
good
long-term
solution.
Okay
and
that's
when
we
have
to
adjust.
J
If
the
community
wants
to
know,
are
we
at
that
point?
I
consider
us
at
that
point
any
time
that
we
have
this
many
patients
with
covet,
and
we
can.
We
can
do
something
demonstrably
to
prevent
people
getting
the
illness.
We
should
be
doing
that.
We
need
you,
owe
it
to
the
people
who
are
taking
care
of
the
patients
in
the
hospital
right
now.
You
owe
it
to
your
friends
and
neighbors
and
your
families
to
do
whatever
you
can
to
stop
the
spread
of
this.
J
A
A
A
A
K
E
K
As
you
know,
the
commissioners
approved
the
release
of
the
rfp
back
in
march
of
2020.
At
that
time,
the
plan
was
include
was
planned
to
be
included
in
the
capital
improvement
plan
for
the
2021
fiscal
year
budget
due
to
cova.
There
have
been
delays,
however.
We
are
prepared
to
release
the
rfp
this
month.
K
A
january
release
would
provide
90
days
for
the
consultant
to
prepare
a
draft
plan
proposal
and
they'll
need
that
time
to
commit
resources
to
meeting
deadlines
and
provide
reasonable
estimates
on
timelines
and
other
requirements
based
on
staff's
feedback
and
the
board's
feedback.
So
after
that,
the
consulting
firm
will
be
selected,
and
I
don't
know
if
I
can't
see
what
you
see,
but
there
was
a
powerpoint
presentation,
is
that
okay,
appointing
a
steering
committee
is
one
of
the
next
steps
in
this
process.
K
So
the
rfp
should
be
released
by
the
end
of
this
month.
Once
that
happens,
we
can
begin
the
process
of
selecting
members
for
a
steering
committee.
That's
something
that
we
would
be
working
with
other
departments
other
boards
to
figure
out
how
that
process
is
going
to
look.
What
type
of
people
will
be
on
that
committee?
How
we'll
do
the
outreach
for
it
certainly
there'll,
be
some
type
of
application
process
and
the
goal.
At
this
point
we
have
a
very
fluid
timeline,
but
the
selection
of
the
applicant
excuse
me
of
the
consultant
could
happen
by
april.
A
L
So
why
are
we
doing
this?
What
are
the
benefits
of
consolidation
both
for
emergency
responders
and
for
the
community?
One
of
the
main
goals
we
have
is
eliminating
that
call
transfer
in
buncombe
county.
If
you
have
a
fire
or
medical
emergency,
you
call
9-1-1,
we
answer.
We
take
your
information,
we
get
you
help.
L
If
you
have
a
law
enforcement
emergency,
it
works
slightly
differently.
You
call
9-1-1.
We
have
to
determine
what
jurisdiction
you're
in.
Are
you
in
the
county?
Are
you
in
the
city?
Are
you
in
woodfin
weaverville
biltmore
forest
black
mountain
mon
tree?
Once
we
determine
that
jurisdiction,
we
will
initiate
a
call
transfer.
We
will
stay
on
the
line
with
you.
L
There
are
multiple
benefits
of
consolidation.
That
is
definitely
our
primary
goal,
but
some
of
the
others
include
staffing
improvements
to
provide
enhanced
coverage
for
24
7
operations,
more
consistent
and
effective
service
delivery.
Obviously,
if
we
reduce
our
call
taking
time,
we
reduce
the
overall
time
it
takes
to
get
response
to
a
citizen
at
their
home.
L
L
L
For
those
of
you
who
don't
know
the
history
of
their
911
center
and
consolidation
in
our
intergovernmental
agreements,
I'll
take
you
through
the
timeline
of
our
history,
pretty
quickly.
In
2003,
we
signed
the
original
intergovernmental
agreement
to
establish
a
consolidated
9-1-1
center
in
2006.
The
first
addendum
to
that
agreement
was
signed.
It
was
a
timeline
extension
in
2009,
the
second
addendum
to
that
agreement
got
signed
that
established
joint
operations
of
the
community
community
center.
L
Sorry
about
that
communications
center
and
essentially
made
buncombe
county
responsible
for
the
cost
of
all
911
equipment
used
to
answer
and
dispatch
calls,
with
the
exception
of
radios
that
are
owned
by
asheville
city
in
2016,
the
north
carolina
911
board
determined
that
the
county
was
co-located
in
2018
buncombe,
county
emergency
services
and
sheriff's
office
dispatch
fully
consolidated
beginning
to
fix
that
process
and
fix
some
of
those
funding
issues
in
2019
the
county
had
to
pay
back
to
the
911
fund.
100.
L
L
L
L
F
A
M
M
Don't
worry
about
too
much,
so
we've
got
some
pretty
aggressive
renewable
energy
goals,
carbon
reduction
goals,
part
of
that
process
for
us
in
the
strategies
that
we're
looking
at
to
to
do
this
to
accomplish
these
goals
is
more
than
just
infrastructure.
I
come
to
you
about
solar,
a
million
times.
We
also
need
to
change
policy.
We
need
to
change
the
way
that
we
make
our
decisions
right
and
so
part
of
that
I
came
to
you
guys.
A
few
months
ago
we
talked
about
high
performance
building
policy
and
lead
gold
policy
for
future
construction.
M
Well,
sustainable
fleet
policy
is
in
that
same
vein,
so
the
purpose
here
is
to
align
our
purchasing
policy
with
our
strategic
plan.
Focus
of
reducing
greenhouse
gas
emissions
give
or
take
about
a
third
of
our
overall
direct
emissions
come
from
our
fleet.
So
this
policy,
just
in
a
nutshell,
says
when
you
purchase
a
new
vehicle
or
when
you
ask
for
a
replacement
vehicle,
we're
going
to
assign
you
the
most
efficient
vehicle
we
possibly
can
in
that
class.
M
M
So
here's
what
that
tier
structure
looks
like
essentially
tier
one
being
an
ev,
a
zero
emission
vehicles
all
the
way
down
to
an
internal
combustion
diesel
engine,
that's
sort
of
the
worst
case
scenario
for
us,
but
we're
basically
saying
we're
going
to
assign
you
a
tier
that
tier
will
be
the
most
efficient
vehicle
in
its
class
and
the
caveat
here
still
meets
operational
needs
right.
That's
really
really
important.
M
If
you
need
a
four
wheel,
drive
pickup,
we're
not
giving
you
a
prius
right,
so
you
know
we're
gonna
make
sure
that
operational
needs
do
take
priority,
but
this
will
help
us
go
in
the
direction
as
we
replace
vehicles
and
ask
for
new
vehicles
of
giving
you
the
most
efficient
one.
We
can
an
avl
pilot
avls
are
automatic
vehicle
locators.
So,
in
conjunction
with
this
new
policy,
we
are
also
implementing
a
pilot
program
to
put
avls
in
some
of
our
vehicles.
M
The
idea
here
is
that
we
hope
to
enhance
the
evaluation
request
process
right,
so
these
avls
basically
give
us
a
ton
of
data
in
terms
of
the
utilization
of
the
vehicles,
their
movement
patterns
potentially
again
looking
at
where
ev
infrastructure
might
make
the
most
sense
for
us
potentially
evaluating
whether
or
not
a
motor
pool
would
make
sense
for
the
county.
We
do
spend
a
whole
lot
of
money
in
mileage
reimbursement
for
employees,
but
the
idea
again
incorporate
zero
emissions
and
low
emission
vehicles
wherever
they're
feasible.
So
it
also
the
another
sort
of
ancillary
benefit.
M
Is
proactive
fleet
maintenance?
Those
little
guys
will
send
engine
codes
to
our
fleet
management
and
say
you've
got
to
check
engine
light.
We
know
it
bring
it
back
to
the
garage,
so
ancillary
benefit
to
those
avls.
So
that's
a
pilot
program
we're
running
sort
of
in
conjunction
with
rolling
out
this
policy
fast,
as
I
could
get
through
that
any
questions.
I'm
happy
to
answer.
M
So
the
what's
coming
out,
gosh
in
like
two
weeks,
I
guess
they're
opening
up
the
rfp
for
level
two
charging
stations
right,
and
so
we
do
have
some
ideas
on
where
we
can
already
put
some
ev
infrastructure.
That
might
make
sense,
especially
in
like
the
downtown
area,
where
we
know
we
have
some
so
we're
not
going
to
be
moving
around.
M
At
the
same
time,
we
are
going
through
the
process
of
doing
the
sort
of
facilities
assessment,
and
so
we
don't
want
to
make
too
many
judgments
on
where
we
can
put
ev
infrastructure,
because
we're
not
entirely
sure
what
the
outcome
of
that
facility's
assessment
might
be.
There
might
be
some
consolidation
of
facilities.
There
might
be
some
new
facilities
proposed,
so
we've
got
our
eyes
on
it
and
we
probably
will
apply
for
at
least
some
level
of
funding.
But
it's
probably
going
to
be
modest.
A
A
It's
an
area
of
rapidly
improving
technology,
so
we
should
be
as
ambitious
as
we
can
to
take
advantage
of
that
from
a
process
standpoint.
Does
the
commission
need
to
vote
to
approve
the
recommended
policy,
or
when
is
I
mean?
This
is
a
great
high
level
overview,
but
is
what's
the
process
for
kind
of
formalizing?
It.
M
To
my
knowledge
up
to
this
point,
it
is
not
a
policy
that
needs
to
be
approved
by
the
board,
so
it
is
a
policy.
That's
already,
we've
already
gone
through
the
process
in
terms
of
the
internal
process,
we
have
the
policy
steering
committee
that
we
have
going
through
the
management
team,
etc.
This
is
more
of
just
an
update
to
the
board
that
this
is
what
we've,
what
we've
come
up
with.
A
Okay,
I
I
don't,
I
think
it's
a
you
know
a
good,
a
good
approach.
I
certainly
wouldn't
be
against
it.
I
mean
I
think
it's
a
good
policy.
I
would
want
to
make
sure
that
we
that
we
stick
to
it.
You
know.
So
it's
a
it's
a
good.
I
think
it's
a
good
long-term
policy,
so
I'm
certainly
not
against
it,
but
I
don't
you
know.
I
think
it's
well
within
your
discretion,
to
be
doing
smart
things
like
this,
so
I
don't
know.
A
I
guess
I
just
asked
the
manager
to
maybe
just
think
about
think
about
that,
but
any
other
questions
for
the
for
jeremiah
right
now,
all
right.
Well,
thank
you.
So
much
great
update,
great
great
work.
Thank
you
all
right.
Jasmine
we've
got
about
35
minutes.
I
do
think
it'd
be
nice
to
have
about
15
minutes
between
the
meetings.
So
do
you
want
to
proceed,
or
do
you
want
to
add
this?
We
could
add
this
to
the
five
o'clock
agenda.
F
F
I
really
appreciated
the
board
engagement
on
a
specific
question.
We
discussed
at
the
budget
retreat,
which
I'll
touch
on
in
this
presentation,
and
my
hope
today
was
to
expand
that
conversation
to
really
get
bored
input
and
perspective
on
the
next
strategic
phase
of
our
work
to
expand
access
to
quality,
early
child
education
and
specifically,
quality
pre-k.
So
this
presentation,
just
is
a
is
a
swim
in
the
shallow
end
of
this
issue,
always
welcome
questions
and
perspective,
and
and
really
look
forward
to
hearing
people's
thoughts
on
this.
F
F
This
set
of
strategies
was
largely
informed
by
the
tremendous
work
of
the
asheville
buncombe
preschool
planning,
collaborative
that
really
set
forth
a
blueprint
for
how
our
community
could
achieve
a
very
significant
scale.
Up
of
early
childhood
education,
particularly
for
three
and
four-year-olds,
and
and
a
very
clear
recommendation
that
as
critical
as
it
is
to
expand
pre-k
doing
that
alone
does
not
address
the
totality
of
issues
that
present
challenges
for
children
and
families
and
that
what
we
really
needed
to
take
was
a
more
holistic
approach.
F
That
included
many
of
the
upstream
factors
that
we
knew
impacted
a
child's
life
by
the
time
they
had
already
turned
four,
and
that's
really
what
informed.
Taking
this
broader
approach,
this
is
doesn't
in
any
way
do
justice
to
the
work
that
both
county
staff
and
fellow
commissioners
in
our
committee
has
done
in
the
last
two
years,
but
just
very
briefly
year.
One
found
us
moving
at
a
very
fast
clip.
F
Commissioner
presley
was
a
pacesetter
he's
our
speedster,
as
we
created
a
committee
developed
systems
for
grant
making
administered
our
first
round
of
grants,
started
doing
site
visits
and
created
data
collection
systems.
In
year.
Two,
this
most
recent
grant
making
period.
We
did
very
focused
efforts
to
increase
the
equity
of
the
grant,
making
process
and
the
actual
grants
that
were
administered
we
improved
and
strengthened
the
grant
making
process.
F
F
One
that
comes
to
mind
immediately
is
a
collaboration
between
verner,
early
learning
and
buncombe
county
schools,
where
verner
is,
is
building
a
new
early
learning
center
on
the
site
of
elementary.
So
there
will
be
a
wonderful
continuum
of
services
and
it's
also
exactly
the
kind
of
collaboration
we
hoped
would
be
fostered
through
county
funding.
F
Another
thing
that
county
funding
has
enabled
this
partnership
to
do
is
leverage
outside
philanthropic
dollars
in
significant
ways,
so
we're
seeing
projects
like
this
really
start
to
coalesce
and
show
the
potential
for
what
this
public
funding
can
achieve,
that
slide's
not
quite
showing
up
there.
But
but
what
you
will
see
in
your
packet
is
just
a
rundown
of
the
grants
we
made
in
2021.
F
You
can
see
the
range
of
grantees
everything
from
asheville
city
schools
and
buncombe
county
schools
to
the
buncombe
partnership
for
children,
to
community
action
opportunities
to
some
smaller
and
more
grassroots
programs
as
well
and
and
see
grant
sizes
ranging
in
size
as
well.
That
kind
of
show
you
the
scope
of
impact
and
what
we're
hearing
from
many
grantees
is
a
lot
of
appreciation.
Certainly
we're
hearing
people
say
that
they're
finally
able
to
put
some
funding
behind
strategies
they've
known
forever,
were
important,
but
that
they
could
never
locate.
F
A
A
F
F
There's
such
a
strong
degree
of
alignment
between
the
strategic
plan
priorities,
especially
around
an
educated
and
capable
capable
community
where
two
of
the
2025
goals
we
establish
include
increasing
kindergarten,
readiness
and
third
grade
literacy.
Two
goals
that,
where
early
child
education
and
pre-k
are
really
instrumental
to
reaching
those,
I
would
I
would
propose,
but
also
see
as
we
look
sort
of
across
the
continuum
of
goals,
that
resident
well-being
and
health
across
the
life
cycle
is
also
an
issue
that,
interestingly,
can
be
impacted
by
access
to
early
childhood
education
and
high
quality
pre-k.
F
There's
a
lot
of
data
showing
that,
so
all
this
to
say
is
there's
a
very
strong
degree
of
alignment
between
strategic
plan
and
and
opportunities
to
continue
our
priority
around
early
child
education.
That
would
include
the
vibrant
economy
piece.
This
is
not
just
about
the
well-being
of
children
and
families,
it's
also
about
the
vibrancy
of
our
local
economic
systems
and
and
the
ability
of
people
to
participate
fully
in
the
workforce
and
our
ability
to
attract
large
employers
who
will
be
looking
for
access
to
quality
child
care
as
one
of
their
top
priorities
for
employees.
F
That
would
be
a
shift
that
would
mean
the
851
000
which,
to
their
great
credit,
asheville
city
schools,
has
been
using
for
their
preschool
program
for
many
years.
They
made
that
decision
because
of
what
a
high
value
they
place
on
preschool
and
that's
certainly
something
we
want
to
support
that
would
preserve
that
and
it
would.
It
would
ensure
that
we
really
had
the
3.6
million
dollars,
plus
the
annual
increase
each
year
to
dedicate
towards
the
expansion
of
programs
and
slots.
F
F
From
a
process
perspective,
the
first
step
is
really
this
board
level
discussion.
The
request
I
put
on
the
table
is
that,
as
a
next
step,
the
board
of
commissioners
basically
extend
a
charge
to
the
early
childhood
education
development
committee,
which
is
to
work
with
county
staff
to
develop
a
set
of
recommendations
for
increasing
access
to
quality
pre-k.
F
That
would
be
informed
by
targeted
equity
strategies
to
reduce
the
opportunity.
Achievement
gap
would
include
longitudinal
research
to
measure
the
actual
impact
of
these
pre-k
programs,
including
around
kindergarten
and
readiness
and
third
grade
literacy,
and
would
include
clear
recommendations
about
the
goal
of
achieving
universal
pre-k
and
whether
that's
something
that
buncombe
county
should
adopt.
F
Based
on
these
recommendations,
I
would
hope
that
this
board
of
commission
after
discussion
and
further
study
could
update
the
october
30th
2018
resolution
so
that
it
most
accurately
reflects
where
we're
headed
in
the
next
phase
of
this
work
and
in
terms
of
a
timeline,
if
the
will
of
the
commission
would
be
to
proceed
in
this
way.
The
proposed
timeline
would
be
that
by
june
of
this
year,
the
early
childhood
committee
would
present
recommendations
to
commissioners.
F
F
H
A
couple
of
initial
thoughts,
and
first
thank
you
to
commissioner
presley
beach,
ferrara
and
white
sides,
and
your
entire
group
who's
worked
so
diligently
in
heart
on
this
really
important
work
in
our
community.
So
thank
you
to
each
of
you
when
I
saw
this
was
on
the
agenda.
I
came
in
with
this
overarching
question
of
what
is
missing
from
our
early
childhood
education
that
we're
not
supporting-
and
I
think
I
may
have
answered
my
own
question
during
this-
and
it's
that
last
recommendation
about
that
goal
of
achieving
universal
pre-k.
H
Should
we
really
consider
having
this
larger
overall
goal
of
we're
going
to
work
over
the
next
x
number
of
years
to
achieve
universal
pre-k
and
then
work
backwards
from
there
with
these
strategies,
because
our
funded
partners
here
have
done
phenomenal
work,
but
should
we
be
thinking
bigger
and
broader
on
this
particular
issue?
So
I'm
going
to
toss
that
back
out
to
y'all,
as
we
continue
this
discussion
to
think
about
what
is
that
really
big
thing
and
how
do
we
achieve
it
from
there.
E
F
N
Afternoon,
commissioners,
I'll
attempt
to
explain
this:
I'm
not
the
budget
director
who
would
do
a
better
job,
but
essentially
to
meet
the
commitment
that
the
resolution
established
of
3.6
million
dollars.
We
added
approximately
2.8
million
of
new
dollars
to
the
budget,
because
we
were
able
to
sort
of
use
this
other
850
000
investment
that
was
already
in
place
in
the
budget
as
part
of
that
as
part
of
the
asheville
city
schools,
education
allocation
toward
that
3.6
million
dollars.
A
E
A
F
And
from
a
process
perspective
the,
why
of
how
that
happened
was
that,
prior
to
2019,
when
this
fund
was
really
created,
county
funding
for
early
childhood
education
was
happening
through
a
lot
of
different
ways,
and
one
of
the
things
that
we
did
was
try
to
consolidate
all
of
those
under
one
umbrella
and
that,
and
so
there
were
some
other
smaller
funding
streams
that
were
also
consolidated.
So
it
was
really
that
consolidation
approach
that
created
that
initially.
I
I
So
we
looked
at
what
was
already
allocated
added
that
and
then
the
difference
is
what
we
added
as
new
money
that
first
year,
and
we
continue
that
really
into
the
second
year.
So
now
we're
asking
the
true
letter
of
the
law
of
the
resolution
was
3.6.
So
that's
the
question.
That's
being
asked
at
the
board
today.
A
A
So
I'm
certainly
supportive
of
that
I
mean,
of
course,
it's
a
pretty
big
new
investment.
I
think
there's
going
to
be
based
on
our
budget
retreat
a
number
of
different
new
investments.
The
commission
is
going
to
want
to
seriously
look
for
ways
to
make
happen
in
this
budget,
and
this
will
be
one
of
them.
A
I'm
sure
we
won't
solve
all
of
our
problems
in
this
one
budget
there'll
always
be
more.
You
know
kind
of
ideas
and
and
needs
than
we're
probably
going
to
have
so
so
the
actual
vote
to
approve
this
recommendation
will
be
part
of
what
we
do
in
our
budget
when
we
formally
vote
on
it
in
june.
Is
that
is.
F
That
your
on
the
funding,
piece,
correct
and
part
of
why
I
want
to
introduce
the
conversation
now
is
that
the
committee
will
be
making
recommendations
based
on
the
amount
that
they
can
award
so
we'll
receive,
grant
applications
in
february
and
then
spend
february
to
april
coming
up
with
a
proposed
portfolio
to
bring
forth
during
the
budget
season.
So
knowing
what
that
watermark
is,
will
allow
the
committee
to
make
the
the
the
have
the
best
informed
process.
A
Okay,
so
so
the
formal
decision
to
approve
additional
funds
won't
occur
until
june,
but
you're
asking
the
commission
if,
if
this
sounds
like
something
we're
really
supportive
of,
could
we
go
ahead
and
signal
that
to
the
staff
so
that
the
they're
they're
planning
to
allocate
that
much
in
the
grants
that
they
receive?
Although
I'll
go,
you
know
again,
none
of
us
can
ever
know
exactly.
What's.
E
F
A
A
A
So
do
we
do
we
have
some
orders
of
magnitude
for
what
we're
thinking
about
realistically,
if
we
were
going
to
do
something
like
that
that
it
would
be
because
I
don't
think
anyone's
gonna,
like
argue
against
the
principle,
but
realistically,
what's
the
order
of
magnitude
of
resources
that
a
community
like
ours,
like
probably
mostly
the
county
commission,
would
need
to
figure
out
to
do
that?
I
mean,
I
don't
know,
maybe
the
maybe
the
maybe
there'll
be
more
federal
resources.
We
don't
know
all
of
that,
but
just
what
could
you
say
about
it
at
this.
F
Point
well,
the
preschool
planning
collaborative
did
a
report
on
this
and
came
up
with
a
number
around
20
million
dollars
that
would
represent
when
you
say
universal,
you
have
to
remember:
there's
always
people
who
won't
opt
in
so
the
goal
being
that
any
family
that
wanted
to
have
access
to
pre-k
could
be
able
to
do
so.
I'm
looking
at
rachel
just
to
fact
check
me
on
on
those
numbers
thumbs
up
on
that.
F
So
you
know
if
the
county
were
to
take
this
step.
It
would
position
us
as
even
more
of
a
leader
around
this
and
would
position
the
county
dollars
we're
investing
really
as
additional
catalyst
dollars.
I
think
so.
Questions
that
would
emerge
would
be
from
that
3.6.
Would
we
want
to
allocate
a
certain
portion
of
that
towards
pre-k?
Specifically,
that's
not
currently
happening.
It's
a
much
more
generalized
approach.
F
A
You
know,
I
guess
I'll
just
you
know
we
need
to
wrap
up
now,
but
thank
you
for
this
presentation.
I
think
this
is
sparking
a
great
conversation.
I
definitely
I
mean.
Does
anybody
here
object
to
asking
the
group
to
come
back
and
we've
got
these
high
level
numbers,
but
to
kind
of
start
you
know
presenting
a
deeper
dive
on
that
I
mean
just
hearing
those
those
those
numbers,
on
the
one
hand,
can
kind
of
seem
discouraging
because
it's
like
gosh.
A
How
would
we
come
up
with
you
know
17
16
million
more
dollars,
but
my
hunch
is
that
once
you
really
start
looking
at
it-
and
you
start
thinking
about
like
it
probably
won't
be,
even
if
we
were
able
to
get
to
that,
it's
probably
not
buncombe
county,
we're
not
doing
that
by
ourself.
Like
you
said,
there's
going
to
be
other
partners
doing
part
of
it.
A
You
know
national.
This
might
be
prior
to
privatized
more
at
a
national
level
which
might
provide
a
lot
of
resources.
It
might
be
more
that
we're
just
contributing
a
relatively
modest
percentage
of
it
and
using
that
to
leverage
a
lot
of
other
things.
I'm
certainly
open
to
like,
let's
really
look
at
it
in
more.
N
C
A
F
Up
on
bringing
this
question
to
the
committee-
yeah,
okay,
yeah,
great,
that's,
very
exciting,
and
and
just
for
the
point
for
purposes
of
clarification
before
we
wrap
are,
is
there
support
or
where
are
we
at
around
this
funding
question
that
just
so
the
committee
can
hopefully
have
the
best
information
available
as
they
head
into
the
grant.
Making
process?
Are
people
comfortable
with
that
tentative
signal
that,
like
the
goal,
would
be
to
increase
the
funding
to
offset
the
tax
amount,
understanding
that
it's
a
dynamic
time
and
that
things
could
change
by
june?.