►
Description
At Wednesday's Board of Supervisors meeting, Drug Court Administrator Melanie Meadows shared the Substance Abuse Committee Steering Committee activity over the last two years with updates, highlights, and vision for the future.
C
Mr
chairman,
members
of
the
board,
dr
casey,
thank
you
all
for
being
for
having
us
here
today.
I
appreciate
the
opportunity
to
be
here
and
to
give
an
update
on
the
many
projects
and
services
that
we
have
going
on
in
the
county
that
address
the
substance
use
issue
by
you.
All's
directive,
back
in
2017,
the
opioid
steering
committee,
was
established
in
response
to
the
heroin
opioid
epidemic.
C
Two
years
ago.
During
my
last
update
to
this
aboard,
we
actually
changed
our
name
to
the
substance,
abuse
steering
committee,
reflecting
a
national
shift
and
drug
trends
that
trickled
down
to
the
states
and
then
to
local
communities,
making
it
important
to
broaden
their
focus
to
all
substance
abuse
and
not
just
heroin
and
opiates.
C
The
scope
of
our
work
is
quite
broad,
as
you
can
imagine,
so
we
developed
three
subcommittees
to
manage
the
workload
you
see,
those
on
the
left
of
the
screen,
prevention
and
education
and
outreach
treatment
and
intervention
and
public
safety,
and
reality,
though,
the
work
of
these
groups
overlapped
tremendously
in
terms
of
activities
and
outcomes.
So
for
purposes
of
our
discussion
today,
I
have
not
categorized
the
work
again.
I'm
pleased
to
be
here
for
two
reasons:
first,
it's
an
honor
to
showcase
our
work,
but
second,
this
is
the
five-year
anniversary
of
the
substance
abuse
steering
committee.
C
So
we
want
to
talk
about
our
successes
over
the
last
five
years.
Our
goal
has
always
been
about
saving
lives
from
the
destruction
of
addiction.
I
know
that
sounds
dramatic,
but
it's
true.
Nevertheless,
we
want
to
keep
people
from
falling
through
the
cracks
making
sure
people
don't
get
lost
in
our
processes
and
in
their
systems.
C
Our
first
step
back
when
we
started
was
to
ensure
that
our
county
workforce,
as
well
as
their
community,
were
educated
with
a
clear
understanding
of
addiction
and
the
various
forms
of
treatment
to
include
an
understanding
of
medications
that
treat
opioid
addictions.
We
provided
the
workforce
and
we
provided
the
community
with
education
opportunities
around
trauma
and
then
the
impact
that
trauma
has
on
addiction,
which
we
all
know
is
quite
tremendous.
C
We
believe
one
of
our
big
wins
is
that
we
have
proactively
worked
to
reduce
the
risk
of
overdose
death
and
offered
assistance
through
outreach
to
those
in
need
back
in
2017
mobile.
We
wanted
to
enhance
mobile
integrated
health
services.
We
wanted
to
be
able
to
engage
individuals
that
had
addiction.
As
you
know,
mobile
integrated
health
does
a
lot,
but
addiction
is
only
one
of
them.
So
what
we
did
was
a
peer
recovery
specialist
was
embedded
in
their
unit.
C
The
peer
recovery
specialist
would
reach
out
to
the
addict
in
need
the
day
of
the
incident
or
the
next
day,
allowing
for
sure
to
turn
around
into
services.
It
was
basically
if,
if
you
will
striking
the
iron,
while
it
was
hot,
getting
the
person
in
need
and
quicker
and
if
they're
willing
connecting
them
to
services
quicker,
resulting
in
a
better
chance
of
long-term
recovery.
C
C
We've
conducted
outreach
to
areas
and
individuals
at
high
risk
for
overdose,
to
distribute
naloxone
and
other
resources.
Naloxone
is
being
distributed
everywhere,
it's
being
distributed
to
community
corrections
during
drug
screens,
it's
being
distributed
at
the
jail
upon
release,
it's
being
distributed
by
ems
staff.
During
their
contacts,
we've
made
a
coordinated
effort
to
distribute
it
at
methadone
clinics
at
churches,
in
the
area
and
in
the
parking
lots
of
hotels
and
the
high-risk
areas
between
may
of
21
and
may
of
22.
C
We've
expanded
our
access
to
medication,
assisted
treatment,
you've
heard
it
referred
to
as
m-a-t
once
we
educated
our
staff.
We
added
additional
nurse
practitioner
hours
in
the
jail
we're
now
able
to
dispense
because
of
the
extra
hours
we're
now
able
to
dispense,
not
only
the
vivitrol
or
the
naltrexone
in
the
jail,
but
also
the
suboxone
or
buprenorphine
in
the
jail.
We
also
have
access
to
methadone
through
community
resources.
So
now
we're
delivering
all
three
fda
approved
forms
of
mat,
where
it's
warranted.
C
We've
also
enhanced
our
outreach
to
the
high-risk
population
in
the
jail
by
embedding
a
clinician
from
mental
health
in
the
jail
to
conduct
assessment
and
provide
treatment,
services
sheriff
leonard.
Of
course,
we
all
know
sheriff
leonard,
is
a
trendsetter.
He
launched
the
smart
program
that
was
just
launched
this
past
month.
In
may,
it
stands
for
supported
medically
assisted
rehabilitative
treatment.
C
This
builds
on
his
success
with
the
heart
program
and
also
allows
for
the
combination
of
cognitive
based
therapies
with
mat
where
warranted
and
supported
and
as
we
all
know,
I
think
we
were
all
there
for
the
premiere
of
the
first
episode
of
jail
house
redemption,
major
kudos
there.
It
was
very
well
received
and
that
series
was
released
last
month
on
discovery
plus
again
we're
trying
to
target
our
highest
risk
population.
That
means
the
jails,
individuals
that
leave
jails
are
between
10
and
40
times
more
likely
to
die
of
an
opioid
overdose
than
the
general
population.
C
So
this
is
especially
high
during
the
three
to
four
weeks
post
release
from
the
jail.
For
this
reason,
we've
been
much
more
intentional
in
our
efforts
to
review
our
processes
to
change
our
policies,
to
educate
the
community
and
staff
all
with
the
intended
goal
of
enhancing
access
to
treatment
and
saving
lives.
We
added
a
full-time
pre-trial
officer
in
community
corrections
to
supervise
individuals
at
high
risk
for
overdose
as
they
depart
the
jail
we've
expanded
our
access
to
medical
medications
for
opioid
use
disorders
and
all
of
their
community-based
services.
That
includes
drug
court.
C
We're
trying
to
build
connections,
I'm
sure
you've,
all
heard
of
a
warm
hand-off
we're
trying
to
ensure
that
the
ball
is
not
dropped
at
any
any
one
access
point
so
that
they
go
from
one
program
or
service
to
the
next
with
is
with
smooth
transition.
For
example,
we
don't
want
an
inmate
to
walk
out
of
the
jail
without
a
next
step,
preferably
that
day
we
don't
want
somebody
to
leave
the
courthouse,
not
knowing
how
to
navigate
their
next
step.
So
we've
got
people
and
places
and
programs
in
place
to
address
that.
C
C
Their
lived
experience
is
useful
for
buy-in
from
the
individual
that
we're
trying
to
connect
to
recovery
and
they
serve
as
an
important
link
to
treatment
and
recovery
support.
All
of
the
county
agencies
that
address
substance
use
issues
in
some
manner
have
expanded
their
use
of
the
peer
recovery
specialists.
I
know
for
drug
court.
The
peer
recovery
specialists
were
crucial
during
the
height
of
covet.
C
We
consider
another
one,
our
overdose
review
committee.
This
is
brand
new.
Well,
six
months,
we
started
it
in
january
of
16..
It
includes
representatives
from
all
of
our
justice
agencies,
as
well
as
mental
health,
fire
and
ems
and
social
services.
We
meet
each
month
and
we
review
three
to
four
individuals.
Who've
recently
overdosed
in
the
county
we're
unique
nationally.
We
are
unique
and
that
we
are
only
not
only
reviewing
the
history
of
fatal
overdoses
but
non-fatal
overdoses
as
well.
C
B
Just
on
that
note,
so
when
you
all
go
through
the
histories
of
those
who
have
had
fatal
overdoses
and
then
non-fatal,
are
you
all
creating
a
universe
of
data,
then
that
is
being
programmed
in
to
allow
you
to
project
more
about
where
certain
needs
might
be
in
in
chesterfield?
I
figured
you
were.
I
just
thought
I'd
ask
that.
C
B
C
C
Thus,
the
importance
of
the
peer
recovery
specialists,
who
kind
of
reach
out
and
try
to
say,
been
there
done
that
we
really
need
to
get
you
locked
into
some
services
and
I
would
say,
and
and
covet
it
slowed
down
a
little
bit
in
the
last
two
years,
but
for
mobile,
integrated
health.
Almost
half
of
the
service
calls
that
the
mobile
integrated
health
team
went
out
on
about
half
of
those
ended
up,
resulting
in
a
referral
to
mental
health
services.
C
So
that
kind
of
brings
us,
because
it
was
a
great
question,
mr
winslow,
because
it
it
this
committee
is
helping
us
identify
where
we
still
have
work
to
do
and
kind
of
brings
us
to
our
next
slide,
which
is
moving
forward
and
looking
ahead.
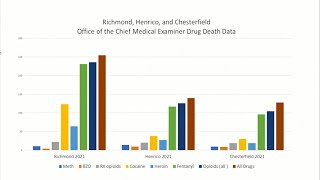
The
data
on
this
chart
reflects
the
number
of
deaths
in
chesterfield
where
substances
caused
or
contributed
to
death.
It
also
shows
what
substances
were
used.
C
It
looks
at
a
calendar
years
from
2016
through
2021.,
it's
a
little
hard
to
see,
but
what
I
wanted,
the
main
takeaway
from
this
slide
to
be
is
that
fentanyl
is
our
greatest
strength
as
our
our
greatest
threat,
certainly
not
our
greatest
strength.
Fentanyl
is
our
greatest
threat.
I'm
probably
not
telling
you
anything
that
you
don't
already
know,
but
this
chart
certainly
validates
it.
It's
not
heroin
it's
fentanyl
and
for
a
long
time
as
a
society,
we
were
laser
focused
on
heroin,
but
we
cannot
singularly
focus
on
heroin
anymore.
C
Fentanyl
is
our
greatest
threat,
because
it's
now
being
combined
with
all
of
the
drugs
this
chart,
as
you
might
expect,
shows
that
we're
not
alone
in
this
we're
not
the
only
locality.
Seeing
this
kind
of
increase-
this
is
for
calendar
year,
2021,
richmond,
chesterfield
and
henrico,
and
you
can
see
the
increase
in
the
abuse
of
fentanyl
fentanyl.
Is
the
green
bar
on
this
chart
everyone's
experience
in
this
increase?
It
has
a
great
deal
to
do
with
the
fact
that
it's
being
mixed
with
other
drugs,
not
just
heroin
strangle.
Yes,
sir.
D
D
B
Why
I
was
asking
the
question
correct,
thank
you
when
the
body
metabolizes
opioids,
like
heroin,
let's
say
with
that's,
been
cut
with
fentanyl
and
I
know
that's
very
common.
Is
that
counted
as
an
opioid
and
can
you
tell
afterwards,
let's
say
the
person
does
disease?
Can
you
tell
if
there's
a
heroin
and
fentanyl
absolutely.
C
C
C
So
what
does
this
mean
for
us
as
we're
moving
forward?
The
substance
abuse
staring
committee,
maintains
contact
and
gets
updates
from
our
work
groups,
and
we
discuss
opportunities
moving
forward.
Every
time
we
meet,
we
have
considered
for
a
moment
a
wish
list,
if
you
will
of
things
that
we'd
like
to
see
satellite
service
sites
at
locations
with
populations
that
are
at
high
risk
of
overdose,
we'd
love
to
establish
an
assessment
center.
C
C
We
will
continue
to
support
our
prevention
and
education
efforts,
our
schools
and
our
schools
in
the
community,
the
psas,
the
podcast,
the
television
and
social
media,
the
resource
cards,
the
narcan
distribution.
All
of
that
will
be
continued,
but
how
do
we
fund
all
of
this
we're
currently
under
a
grant
a
cosap
grant
that
will
carry
our
positions
for
the
next
few
years,
but
we
are
going
to
continue
to
seek
grants
and
long-term
funding
streams.
C
One
such
stream
we're
keeping
an
eye
on
is
the
virginia's
opioid
abatement
authority,
which
will
be
administering
our
share
of
any
legal
settlements
or
judgments
that
were
related
to
the
manufacturing
and
the
marketing
and
sale
and
distribution
of
opioids.
As
we
all
know,
mr
holland
is
one
of
the
chosen
to
serve
on
that
11-member
panel.
We're
hopeful
that
those
funds
will
be
significant
enough
to
offer
us
some
long-term
solutions
and
not
just
some
short-term
fixes,
some
long-term
solutions
and
we
are
going
to
be
ready
and
waiting
with
a
list
when
we
get
there.
E
A
E
Or
take
questions,
mr
chairman,
if
I
may,
I
just
want
to
thank
you
for
mentioning
that.
It's
a
great
segue
for
me
to
say
to
you,
as
a
member
of
the
the
oaa
committee,
we're
well
on
our
way
to
having
our
director,
which
we
expect
within
the
next
couple
of
weeks
we're
going
to
be
hiring
a
new
finance
director,
along
with
the
new
executive
director,
so
we'll
we're
well
on
our
way
to
moving
forward,
and
you
can
see
some
funding
streams
I
think
before
this
year
ends.
So
I'm
excited
about
that
aspect.
E
I
was
going
to
suggest,
and
you
you
have
great
ideas
and
comments
here
which
is
excellent,
was
that
I
welcome
your
suggestions
and
ideas
to
us
so
that
we
can
work
with
our
new
director
to
get
the
resources
moving
to
solve
the
crisis
and
to
work
with
you.
So
we're
excited
about
that
and
I'm
very
excited
to
share
that
we're
well
on
our
way
and
the
money
is
on
the
way.
E
Just
let
us
know
where
you
need
it,
what
you
need
and
it's
gonna
we're
gonna,
do
it
do
it
just
for
that
this
purpose.
So
thank
you.
So
much
for
it,
but
also
thank
you
for
your
leadership
in
this
area.
I've
done
tremendous
job
over
the
last
several
years,
five
years
as
you
mentioned,
and
so
we
applaud
you
and
thank
you
for
that,
and
always
I'm
always
available
to
you
know
24
7
as
well.
Anything
I
can
do
to
help,
and
certainly
through
the
authority,
I'm
honored
to
serve
and
humble
that
as
well.
Thank
you.
A
Mr
karen,
thank
you
going
back
to
one
of
the
other
slides
when
it
shows
the
numbers
by
for
drug
examiner
deaths
for
fentanyl
and
heroin
in
all
drugs
is
this.
Are
we
is
this
showing
that
I
think
the
number
is
19
heroin
deaths,
but
isn't
true
that
it's
pretty
common,
that
heroin
is
being
actually
cut
with
fentanyl,
which
is
probably
what's
causing
the
overdoses.