►
Description
No description was provided for this meeting.
If this is YOUR meeting, an easy way to fix this is to add a description to your video, wherever mtngs.io found it (probably YouTube).
A
Good
morning
welcome
to
meeting
number
three
of
the
house
budget
review
subcommittee
on
health
and
family
services.
As
a
reminder,
remote
access
is
allowed
to
all
meetings
for
the
2022
regular
session.
Members
were
provided
a
zoom
link
to
access
the
meeting
remotely
the
meeting
materials
were
put
online
earlier
this
week
and
made
available
for
downloading.
A
A
D
You,
mr
chair,
I
just
looked
out
in
the
audience,
and
I
saw
commissioner
brian
painter
is
here
with
us.
Thank
you
for
being
here,
and
I
know
that
the
kentucky
medical
association
is
here
today
talking
to
a
lot
of
folks.
I
don't
know
if
we
have
anyone
here
in
the
room,
but
thanks
for
being
with
us
today,.
A
Okay
and
I
want
to
introduce
keith
watts,
he's
the
county
commissioner
from
boyd
county
back
there
in
the
middle.
Thank
you
keith
for
being
here.
I
know
how
long
you
drove
because
I
drive
it
every
week.
So,
okay,
we've
had
the
approval
minutes
and
before
we
get
begin
with
the
presentations
for
members
participating
remotely,
please
remember
to
meet
your
microphone.
A
We
have
a
full
agenda
with
several
presenters.
This
morning.
First
we
have
commissioner
lee
and
mr
steve
bechtel
from
the
department
of
medicaid
services
to
give
us
a
presentation
on
the
governor's
medicaid
budget
recommendations.
Members.
Please
hold
your
questions
until
after
the
presentation,
please
and
we'll
take
questions
from
members
in
the
room
and
then
questions
for
the
members
participating
remotely
presenters.
Please
identify
yourselves
for
the
record.
E
G
E
And
we're
very
pleased
today
to
be
here
to
talk
to
you
about
the
medicaid
budget,
and
while
this
is
definitely
a
team
presentation,
I'd
like
to
acknowledge
that
mr
bechdel
is
actually
the
one
who
did
the
heavy
lift
of
pulling
all
of
this
information
together
and
worked
tirelessly
to
make
sure
that
we
had
a
very
good
presentation
to
deliver
to
you
today.
So
sarah,
if
we
could
go
to
the
first
slide,.
E
So
first,
we
just
want
to
give
you
a
little
overview
of
medicaid
at
a
glance
we
have
currently,
whereas
of
december
2021
1.6
million
individuals
enrolled
in
the
program.
As
you
can
see
from
the
numbers
listed
here,
the
bulk
of
those
individuals,
almost
1.1
million,
are
in
the
traditional
category,
which
includes
aged
blind,
disabled
pregnant
women
and
children.
We
have
another
590
000
covered
under
our
medicaid
expansion.
E
We
have
approximately
5
59
300
providers
enrolled
in
delivering
services
to
the
population
we
serve,
and
our
budget
in
2021
was
14.6
billion
in
expenditures
that
included
both
administrative
and
benefit
combined
next
slide.
Sarah,
so
the
budget
for
the
medicaid
program
is
has
two
basically
two
categories:
our
benefits
budget,
which
is
services
delivered
to
individuals
enrolled
in
the
program.
It
does
include
mandatory
and
optional
services.
E
It
also
includes
capitation
payments
that
we
make
to
our
managed
care
organization
and
our
non-emergency
medical
transportation
program,
and
then
we
have
some
below
the
line
line
items
such
as
pharmacy
rebates,
medicare
premiums
that
we
pay
for
individuals
who
are
dually
eligible.
We
also
have
some
potential
funding
for
additional
budget
requests.
Their
administrative
budget
consists
of
contracts.
E
E
So
dms
receives
various
levels
of
funding
from
cms
the
center
for
medicare
medicaid
services,
based
on
the
specific
activity
being
conducted,
for
example,
most
of
our
administrative
costs
for
personnel
certain
contracts.
We
receive
a
50
federal
fmap
from
cms
for
those
services,
as
we
mentioned
just
previously,
our
advanced
planning
documents
submitted
to
cms.
E
We
also
receive
an
enhanced
match
for
a
skilled
professional,
such
as
pharmacists
and
nurses,
and,
as
you
can
imagine,
kentucky
is
experiencing
the
same
issues
as
their
providers
in
trying
to
recruit
and
retain
nurses
due
to
the
competitive
nature
and
and
costs
related
to
those
services.
So
again,
we
are
in
the
same
same
situation
as
others
trying
to
recruit
and
retain
nurses
in
our
program
next
slide,
and
this
is
just
a
scenario
of
our
administrative
budget
and
it
includes
cost
of
living
adjustments.
E
Implementation
of
a
basic
health
plan,
which
is
a
plan
that
will
serve
as
a
safety
net
for
individuals
who
are
currently
falling
through
the
cracks,
for
example,
they
don't
qualify
for
medicaid
and
they
can't
get
a
product
on
the
exchange.
So
we
believe
that
basic
health
plan
is
going
to
continue
to
provide
a
continuum
of
care
for
individuals
in
the
in
the
commonwealth.
E
E
So
the
benefits
budget
is
developed,
you
can,
as
you
can
see
there,
it
was
a
collaborative
effort
and
a
lot
of
work
goes
into
predict
projecting
the
budget.
The
collaboration,
of
course,
is
between
cabinet
officials,
governor's
office
and
the
state
budget
director.
We
use
definitely
historical
data
to
develop,
managed
care
capitation
rates.
We
also
use
enrollment
projections
to
to
determine
how
much
funding
we
will
need
going
forward,
and
then
the
final
product
from
this
is
the
consensus
forecast
that
makes
up
the
benefit
budget
next
slide.
E
And,
as
you
can
tell
from
our
benefit
budget,
we
do
receive
certain
fmap
or
medical
as
assistance
percentages
from
the
centers
for
medicare
and
medicaid
services
for
the
individuals
that
we
serve
traditionally
medicaid
receives
about
75
or
70
f
map,
as
you
can
tell
there's
a
blended
rate
you
can
see
from
for
2022,
going
to
2024
that
that
f
map
changes
a
little
bit
likewise
with
chip.
Typically,
it's
around
eighty
percent,
so
the
traditional
medicaid
f
map
and
the
chip
f
map
are
flexible.
E
F
F
The
one
thing
that
we
will
comment
on
is
in
22.
In
the
budgeted
we
will
be
asking
a
current
year:
appropriation
increase
as
you,
you
may
already
know,
of
709.1
million
federal
fund
appropriations,
and
the
reason
for
that
is
the
6.2
f
map.
When
we
did
the
22
budget,
we
assumed
that
the
6.2
f
map
was
would
be
ending
that
the
public
health
emergency
would
have
ended,
so
we're
just
asking
for
those
funds
and
those
appropriations
to
be
replenished
next
slide.
Please.
F
F
For
for
that,
for
those
initiatives
and
those
initiatives
included,
those
are
in
section
20.
I
believe
subsection
20
of
the
benefits
budget
in
house
bill,
1
substitute
one
and
those
it's
basically
a
ten
percent
across
the
board
rate
increase
for
five
of
our
waivers
one
waiver
that
was
excluded,
I
will
say,
was
model
model,
2
waiver,
but
all
the
other
waivers
were
to
receive
a
10
across
the
board
rate
increase
for
all
services.
F
E
And
one
thing
one
thing
I
would
like
to
add
about
the
10
across-the-board
increase
for
those
waiver
provider
types.
Currently
there
are
some
inequities
in
the
reimbursement
for
particular
services
across
waiver
providers,
so,
for
example,
one
provider
may
receive
a
different
funding
and
for
for
services
for
the
same
service
provided
in
a
different
waiver.
So
we
believe
that
a
10
across
the
board
raised
for
those
providers
would
also
still
result
in
inequities
across
the
waiver
types
and,
as
you
know,
there
has
been
a
lot
of
focus
on
waiver
redesign.
F
And
to
further
to
go
into
that
further
cms
requires
an
approved
justifiable
rate
methodology.
So
when
we
do
a
10
across
the
board,
we're
gonna
have
to
submit
pretty
much
waiver
resubmissions
and
amendments
for
every
one
of
those
five
waivers
and
a
part
of
that
they'll.
The
cms
will
require
us
to
provide
supporting
documentation
of
the
methodology
used
to
derive
the
10
percent
figure.
F
So
how
did
we
come
up
with?
10
is
10
adequate
and,
like
the
commissioner
said,
you
know,
cms
will
be
concerned
about
the
parity
that
that
this
10
percent
across
the
board.
These
types
of
increases
do
not
address
parity,
so
we
have
to
address
the
parity.
We
have
initiated
a
rate
study
across
all
of
our
waivers,
but
that
rate
study
is
not
scheduled
to
be
completed
until
later
this
fall
and
then
the
last
thing
on
this
slide
is
appendix
k,
a
part
of
a
section
20..
F
It
talks
about
taking
the
residential
cost
up
to
like
50
percent
of
the
appendix
k
rates.
When
the
pin
mix
k
expires,
some
of
these
rates
will
decrease
upon
the
end
of
the
public
health
emergency
and
when
the
public
health
emergency,
the
appendix
k
sunsets,
so
the
rates
the
rate
increases
for
these
will
not
qualify
for
federal
funding
and
will
need
to
be
supported
with
state
general
funds.
F
F
You
know
once
we
get
that
that
approval,
if
we
can
get
that
approval,
like
I
said
earlier
of
using
that
in
a
spending
plan
of
an
updated
spending
plan,
the
the
other
thing
is
without
the
increase
described.
The
described
above.
The
fiscal
analysis
indicates
that
the
current
funding
that
was
provided
in
sections
18
and
19
of
house
bill
1
for
the
sel
and
michelle
p
slots
may
be
a
little
a
little
low,
and
this
is
why
you
got
43
what
we
feel
is
for
seo.
F
We
can't
say
it
enough.
Current
language
in
the
house
bill
says
that
we
will
use
the
arpa
funds
from
to
to
to
help
fund
these
rate
increases.
But
this
again,
this
type
of
rate
increase
was
not
included
in
the
approved
spending
plan.
I
can
tell
you
we,
I
believe
the
spending
plan
was
approved
in
september
of
2021
and
we've
been
working
toward
implementing
those
things.
Since
then,
so
we
will
that
that
is
a
challenge,
and
that
is
concern
of
ours.
F
F
If
cms
does
not
approve
the
10
rate
increases
the
way
the
language
is
today,
we
could
be
lawfully
required
to
to
still
proceed
forward
with
these
rate
increases
without
cms
approval
and
what
that
means.
That
puts
the
state
at
a
great
financial
risk,
because
all
those
funds
would
be
state
funds
only
so
that
that
was
the
last
piece
of
the
slide
and
one
other
thing
I
will
say:
is
we
we're
monitoring
and
we're
aware
of
a
lot
of
legislation?
That's
coming
through.
F
Just
just
want
to
point
out
that,
once
we,
when
we
see
those
bills
pass,
they
got
a
price
tag
if
it's
an
increased
rate,
if
there's
an
increase
in
rates
or
an
increase
in
services
provided
by
medicaid,
it's
going
to
be
a
price
tag
to
that,
and
the
budget
that
we
presented
here
today
was
what
it
is
doing
business
as
of
today.
So
anything
that
you
may
see
across
your
desk
or
that
we
may
see
that
comes
across.
E
C
Thank
you,
mr
chairman,
so
I
guess
my
question
is
you
always
have
concerns?
Have
you
who
have
you
talked
to
have
you
talked
to
chair,
petrie
or
reed,
or
anybody
in
the
senate
or
about
these?
It
sounds
like
you.
You
don't
want
that
money
because
of
the
issues
that
might
arise,
and
I
understand
that
I
understand
your
concern
from
what
you've
presented.
Who
have
you
talked
to
to
try
to
rectify
it?
C
G
I
have
been
in
contact
with
chairman
petrie.
He
has
agreed
that
we
will
continue
to
be
on
those
discussions.
He
was,
I
believe,
appreciated
appreciative
that
we
brought
this
to
his
attention
and
I
I
always
I
always-
and
I
want
to
say,
appreciate
how
well
we've
been
able
to
work
together
on
these,
and-
and
I
didn't
want
to
surprise
anybody
with
this.
So,
yes,
we
we
have.
We
have
let
folks
know.
B
Thank
you,
mr
chairman
yeah,
thank
you
for
the
presentation
and
thank
you
for
the
work
that
you
do.
This
is
a
question
about
the
waiver
slots
and
in
the
smi
task
force.
One
of
our
main
recommendations
was
a
dedicated
waiver
for
medicaid
waiver
for
supported
housing
for
people
with
severe
mental
illness
and,
as
you
know,
I'm
sure
you
know
it's
the
only
category
of
disabled
adults
that
don't
have
a
dedicated
waiver,
don't
qualify
for
a
current
waiver.
Is
that
issue
something
that's
on
your
radar?
B
E
Is
something
that's
definitely
on
our
radar
deputy
commissioner
leslie
hoffman
is
heading
up
this
initiative
and
she
has
been
talking
to
cms
related
to
incorporating
an
smi
piece
into
one
of
our
existing
waivers.
Cms
believes
that
may
be
the
easiest
route
to
go
so
definitely
on
our
radar
and
as
we
get
more
information
and
would
definitely
be
happy
to
to
give
that
information
to
this
committee.
A
B
Thank
you
chairman,
thank
you
for
being
here
with
us
today
and
I
just
have
a
clarification
question,
because
I
just
want
to
make
sure
that
I'm
understanding
it
correctly,
but
other
states,
including
wisconsin,
have
implemented
across
the
board
rate
increases,
and
did
you
claim
that
that
was
not
a
possibility?
I
just
wanted
to
get
some
more
information
in
that
area.
H
E
G
And
commissioner,
isn't
the
other
clarification
that
under
appendix
k
there
is
additional
flexibility
there,
but
we
have
to
rewrite
our
plan
for
appendix
state
to
allow
that
and
some
states
have
done
that.
But
when
appendix
k
goes
away
then
you
can't
support
that
additional
10
percent
moving
forward.
And-
and
so
it's
an
it's
a
nuanced
response
to
your
question.
But
that's
those
are
kind
of
all
the
components
that
go
into
it.
I
Thank
you,
mr
chairman.
I
have
a
few
questions
and
then
a
few
comments.
If
that's
okay,
okay,
first,
if
you
can,
can
you
all
just
bring
it
bring
it
over
to
us
or
send
it
over
to
us?
Can
you
all
provide
the
math
to
all
to
the
1915
rate
increases
and
the
estimates,
if
you
all,
can
provide
that
over
to
the
chairman
petra
in
my
office?
If
you
can,
I
appreciate
that
another
thing
is
last
spring.
You
all
testified,
chfs
needed
a
funding
for
the
waivers.
I
E
I
don't
think
that
we're
opposed
to
rate
increases.
We
want
to
make
sure
that
the
rate
increases
are
fair
and
equitable
across
the
board,
and
again
cms
has
stated
that
we
need
a
an
improved
rate
methodology
before
going
forward
with
increasing
those
rates.
So
we
are
definitely
not
against
rate
increases
for
our
waivers.
G
And
let
me
be
even
more
equivocal
than
that
we
are
for
rate
increases
for
our
waiver
providers.
We
absolutely
know
they
need
the
support.
Absolutely.
What
we're
saying
is
we
need
to
be
sure
that
the
funding
is
there
so
that
you
don't
put
medicaid
or
future
budgets
at
risk
and
we're
just
trying
to
give
you
what
we
see
as
the
numbers
which
will
supply
you
on
what
those
would
cost.
E
E
G
There
are
long
waiting
lists,
they're
long
waiting
lists.
We
know,
we
know
the
demand
is
there
and
we
believe
we
can.
We
believe
the
staff
is
there,
but
it
is
a
good
point.
Personnel
pressures
across
healthcare
are
are
going
to
present
a
challenge
I'll
talk
to
about
child
care
this
morning
and
it's
the
same
challenge.
That
personal
challenge
is
a
very
real
challenge.
I
A
A
J
J
J
J
One
in
seven
senior
citizens
are
food
insecure
at
this
time,
and
35
percent
of
kentuckians
have
a
disability
with
the
main
number
one
disability
being
ambulation
and
then
again,
over
a
million
individuals
are
age,
60
or
older
in
kentucky,
and
we
are
honored
and
proud
to
serve
them
next
slide
you'll
see
here
that
our
funding
comes
through
federal
and
state
general
fund
streams
and
just
wanted
to
give
you
an
idea
as
to
what
federal
funds
are
used
to
provide
services.
To
many
of
you
are
aware
of
our
long-term
care
ombudsman
program.
J
Additionally,
many
of
you
all
are
very
familiar
with
our
senior
center
senior
citizen,
centers
and
our
home
delivered
meal
programs,
and
some
of
that
funding
does
come
through
federally
through
the
older
americans
act.
Additionally,
we
ensure
that
older
adults
have
an
opportunity
to
learn
about
disease
and
have
strategies
to
prevent
disease
and
also
promote
healthy
living.
J
We
also
strive
to
ensure
that
any
older
adult
age,
60
or
older
who's
interested
in
returning
back
into
the
workforce
has
training
opportunities
and
connections
to
do
so.
Additionally,
we
ensure
that
older
adults
that
are
living
in
their
community
have
the
supportive
services
that
they
need
so
that
they
can
continue
to
live
independently
in
their
community.
Supportive
services
include
in-home
aids
yard
work,
some
home
repairs
and
transportation.
J
This
is
a
list
of
the
different
state
general
funded
programs
that
the
department
for
aging
and
independent
living
oversees
you'll
see
here
that
we
provide
services
for
individuals
with
traumatic,
brain
injury
as
well
as
to
their
family
and
caregivers.
We
certify
assisted
living
communities.
There
are
about
120
assisted
living
communities
across
the
state.
J
We
also
utilize
state
general
funds
to
provide
services
for
individuals
with
disabilities.
Specifically,
our
personal
care
attendant
program
provides
services
to
individuals
with
the
loss,
the
functional
loss
of
two
or
more
limbs.
So
if
you
think
of
someone,
that's
had
a
spinal
cord
injury,
a
stroke
or
amputations.
J
We
also
oversee
the
heart,
supported
living
program
and
home
care
program
that
aim
to
provide
services
and
our
program
of
last
resort,
and
what
that
means
is
that
individuals
that
apply
for
these
programs
have
to
ensure
that
they
don't
meet
medicaid
qualifications
and
that,
if
they
do,
they
can
receive
the
same
services
through
medicaid
waiver.
If
not,
then
they
can
receive
services
through
our
state,
general
funded
programs
and
then
also
we
oversee
a
family
caregiver
program.
This
program
is
specifically
aimed
to
supporting
grandparents
raising
grandchildren
only.
J
J
Additionally,
we
provide
oversight
for
the
state
independent
living
council.
The
state
independent
living
council
is
made
up
of
individuals
across
the
state
that
work
closely
with
our
centers
of
centers,
for
independent
living,
to
ensure
that
individuals
with
disabilities
have
a
voice
and
have
community
access
and
are
able
to
engage
in
their
community
successfully.
J
One
of
the
things
we
were
able
to
do
was
to
establish
the
first
ever
health
occupation,
students
of
america,
partnership
with
our
area
agencies
on
aging
and
independent
living.
What
that
meant
was
we
were
able
to
connect
high
school
students
who
were
interested
in
going
into
a
healthcare
healthcare
field
with
individuals
that
are
aging
out
in
their
community.
This
was
significantly
successful
out
in
the
purchase.
J
Additionally,
through
this
partnership,
some
of
the
local
businesses
donated
funds
or
materials
to
help
support
this
initiative.
We
have
had
the
honor
to
go
and
present
on
this
partnership
opportunity
nationally
and
to
teach
other
states
as
to
what
we're
doing
here.
In
april
of
last
year,
I
had
the
opportunity
to
go
down
to
purchase
and
connect
with
the
graves
county,
high
school
and
mayfield
technical
school,
and
we
were
able
to
go
out
and
some
of
the
high
school
students
were
able
to
meet
their
senior
citizens
for
the
first
time.
J
We
also
implemented
the
shot
of
hope
at
home
within
the
department
for
aging
and
independent
living.
We
are
one
of
the
first
states
to
vaccinate
homebound
individuals
with
the
kobit
19
vaccine.
It
is
something
I
am
so
proud
of,
and
it
really
took
multiple
partnerships,
especially
within
the
kentucky
department
of
public
health,
but
to
ensure
that
our
individuals
that
were
homebound
had
a
true
shot
of
hope,
also
partnered,
with
the
kentucky
national
guard
to
implement
this
as
well.
J
J
Again,
this
is
an
opportunity
for
individuals
with
disabilities
to
ensure
that
they
have
individuals
that
they
can
direct
to
assist
in
their
care,
whether
it's
personal
care
or
community
integrated
services
and
then.
Lastly,
as
many
of
you
know,
we
have
been
able
to
eliminate
the
wait
list
for
senior
meal
services
statewide.
J
J
You
will
note
in
2020
about
61
of
our
funding
came
from
general
funds
with
an
overall
expenditure
of
71
million
dollars
and
you'll
notice,
as
we
go
through
the
slides
that
that
starts
to
change
in
fiscal
year
21
we
were
about
50
50
dependent
on
general
funds
and
federal
funds
in
part,
you'll
see
a
significant
increase
in
federal
funding,
and
that
is
due
to
all
of
the
different
federal
funds
received
with
arpa
pairs,
ffcra
a
multitude
of
acronyms
and
then
in
fiscal
year.
22
is
really
when
it
starts
to
change.
J
J
There
is
a
request
for
7.2
million
for
the
current
fiscal
year
to
continue
to
provide
meals
at
an
unprecedented
rate
and
then
29
million
over
the
next
two
fiscal
years
in
order
to
ensure
so
I'm
sure
many
of
you
are
asking
what
happens
if
we
don't
have
that
money?
What
happens
is
is
that
we
have
to
there
for
about
2,
000
seniors
that
are
currently
receiving
meals.
We
would
have
to
place
them
back
on
a
wait
list
or
find
some
other
alternate
plan
for
them
to
receive
services.
J
J
It
would
not
be
possible
to
deliver
the
exponential
number
of
meals
that
we
have
delivered
over
the
past
year
without
our
volunteers.
So
thank
you
and
want
to
leave
you
all
with
one
last
thing
regarding
senior
meals,
maxine
from
stanford
kentucky.
I
wanted
you
all
to
know
that
she
loves
receiving
the
meals
and
also
seeing
the
smiling
faces
that
deliver
the
meals
to
her
each
week.
J
J
Without
those
grant
funds
the
office
will
not
be
able
to
continue
to
operate.
Additionally,
there
is
additional
funding
requests
for
our
heart
supported
living
program.
This
is
a
program
that
provides
support
for
individuals
and
families
that
have
disabilities.
Again,
it
is
a
program
of
last
resort.
J
J
That
is
what
they
have
shared
with
us
and
then,
lastly,
is
the
national
core
indicators
program
to
support
aging
and
disability.
This
is
a
program
that
is
held
at
the
national
level.
Currently,
our
sister
agency,
the
department
for
behavioral
health,
developmental
and
intellectual
disabilities,
participates
in
this,
and
this
is
a
quality
support
initiative
and
it
ensures
that
individuals
receiving
services
that
they're
receiving
quality
services
and
allows
consumers
to
have
a
voice
next
slide.
J
J
Some
of
you
all
who
have
been
here
for
a
while
know
that
the
cabinet
has
worked
so
hard
to
try
and
get
pace
up
and
going
getting
pace
started
was
started
under
governor
bevin's
administration
and
we've
carried
it
through
under
governor
beshear's
administration
and
fingers
crossed.
We
will
be
opening
up
our
the
first
couple
pace
centers
later
this
year
and
are
so
excited.
J
Pay
serves
individuals,
age,
55
and
older
that
are
dual
certified,
medicaid
and
medicare,
and
just
really
excited
for
this
opportunity.
We
are
also
at
developing
and
implementing
our
statepoint
on
aging
dashboard.
Our
federal
state
plan
on
aging
was
approved
last
year
and
we're
going
to
be
implementing
a
dashboard
to
track
the
goals
to
ensure
that
we
are
moving
kentucky
forward
and
being
innovative
and
creative
with
many
of
our
community
partners
to
support
our
aging
community.
J
We
also
have
received
a
five
million
dollar
administration
on
community
living
grant
to
support
individuals
with
brain
injury,
and
so
we
are
partnering
with
many
of
the
universities
and
other
associations
across
the
state
to
launch
a
reap
program.
Reap
stands
for,
remove,
reduce,
educate,
adjust,
accommodate
and
pace.
It's
really
focused
on
ensuring
that
students
who
have
a
concussion
can
return
back
to
school
and
have
the
services
that
they
need
to
support
them
as
they
go
through
their
concussion
management
program.
J
J
C
C
J
It
does
not
it
states
specifically
that
if
individuals
are
eligible
for
kinship
care,
they
have
to
go
kinship
care
first.
In
being
completely
honest
with
you,
the
state
funded,
the
state
funded
family
caregiver
program
has
had
significant
cuts
to
it.
Over
the
past
couple
years
it
went
from
a
1.9
million
dollar
program
down
to
a
534
thousand
dollar
program.
So
in
fiscal
year
18
we
were
serving
632
grandparents,
and
this
last
fiscal
year
we
served
200.
C
C
D
J
Sure
that
that's
a
great
question,
so
we
offer
supportive
counseling
and
ensuring
that
grandparents
attend
support
groups
and
are
aware
of
all
the
services
available
to
support
them
in
their
community.
In
addition
to
that,
there
is
a
stipend
that
they
receive.
It's
a
500
stipend
that
they
receive
many
of
the
grandparents
receive
custody
and
don't
know
what
to
do.
Don't
have
bedding
clothing,
the
specific
items
to
support
individuals,
and
so
there
is
a
stipend
that
they
can
receive
to
purchase
to
purchase
items
to
support
their
grandchildren.
D
A
D
J
So
I
can
share
with
you
specifically.
The
budget
request
is
for
482
thousand
dollars
each
fiscal
year.
It
is
specifically
to
ensure
that
the
office
continues
to
fund
for
our
director.
Our
director
is
jennifer
craig.
She
has
started
in
october
and
has
been
just
whitening
in
a
bottle.
She
is
wonderful.
The
legislation
that
was
passed
also
stated
that
the
office
should
have
a
director
and
administrative
support
person
through
there
was
not
funding
tied
to
to
that
piece
of
legislation.
J
There
are
many
other
states
that
have
a
well-established
office
to
the
point
at
which
many
of
them
have
office
of
dementia
services
regional
coordinators
across
their
their
region.
South
carolina
is
one
that
is
really
stands
out
as
well
as
georgia,
so
they
were
all
really
excited
to
hear
that
kentucky
is
moving
forward
on
this
and
are
happy
to
provide
any
assistance.
G
D
When
we
were
discussing
the
legislation
and
talking
with
the
cabinet
it,
it
was
my
understanding
that
part
of
the
reason
for
really
getting
this
office
up
and
running
was
to
be
able
to
apply
for
more
grants.
So
I
understand
that
you
are
operating
under
a
grant.
That
expires
in
2024
is,
is
the
grant
writing
process
also
part
of
the
the
funding
stream?
D
J
What
we
are
only
asking
for
is
for
the
personnel
cost
to
cover
that
office,
so
the
office
of
dementia
services
coordinator
is
actively
working
on
seeking
out
other
grant
opportunities
to
specifically
continue
to
provide
services
to
individuals
as
well
as
she
is
looking
for,
grant
opportunities
to
support
her
position,
but
her
main
goal
right
now.
One
grain
that
we
do
have
is
called
bridging
the
gap.
J
It
is
a
million
dollar
grant
to
support
individuals,
specifically
older
children,
that
are
caring
for
their
parents,
that
have
dementia
and
helping
them
navigate
the
waters
and
ensure
that
they
have
what
they
need
to
live
in
their
home.
So
again,
the
funding
would
be
specifically
for
that
position
only
and
then
the
director
and
support
staff
would
go
after
other
grant,
opportunities
to
support
kentuckians
and
their
in
their
individuals
with
dementia.
D
Okay,
I'm
I'm
just
trying
to
understand
the
482
thousand
dollar
per
year
number,
because
when
we
talked
about
the
legislation
the
ask
was-
or
the
estimate
was
approximately
150
000
per
year
for
staffing
that
office.
So
I'm
I'm
not
exactly
clear
on
on
what's
happening,
but
I
applaud
your
efforts.
I
I
know
it's
necessary.
D
Hopefully
we
can
keep
that
number
from
expanding
and
growing
in
our
in
our
budget
requests
and
just
one
last
thing,
I'm
very
glad
to
see
that
the
guardianship
modernization
is
happening.
I've
had
some
personal
care
homes
in
my
district
who
have
had
a
really
difficult
time
getting
answers
on
guardianship
from
some
of
their
residents
and
it
interferes
with
their
ability
to
be
paid
to
the
tune
of
about
two
years
so
very
necessary.
A
A
H
H
In
our
state,
in
the
state
of
kentucky,
we
have
219
024
children
that
are
defined
as
having
a
special
health
care
needs,
and
that
is
basically
a
child
who
receives
more
needs,
more
care
than
the
average
child,
or
maybe
they're
on
medications
or
they
they're
enrolled
in
occupational
therapy.
Physical
therapy
speech
therapy,
whatever
that
is,
we
have
219
000
children,
so
we
try
to
meet
those
needs
through
indirect
care,
indirect
services
and
collaborations
with
partners
across
the
state.
H
So
it's
a
direct
care
service.
If
you
go
to
the
next
slide,
please
so
we
have
clinics
across
the
state.
We
have
eleven
different
districts.
We
collaborate
with
providers
across
the
state
we
contract
with
providers
within
our
own
office.
We
have
nurses,
we
have
social
workers,
we
have
administrative
staff,
we
have
audiologists
in
each
of
those
offices
and
then
again
we
collaborate
in
order
to
ensure
that
we're
seeing
all
of
those
children
and
ensuring
that
those
the
most
vulnerable
in
our
state
are
receiving
services.
H
H
So
you're
probably
familiar
with
our
medical
clinics.
We
have
specialty
medical
clinics.
We've
had
these
clinics
for
for
years,
but
one
of
the
things
that
occurred
during
the
pandemic.
Coping
19
is
our
telehealth
services,
so
we
shifted
from
telehealth.
We
had
probably
about
423
over
a
period
of
six
months
prior
to
the
pandemic,
to
that
we
looked
at
that
same
six
months
and
it
increased
to
over
1200,
so
the
telehealth
visits
increased.
H
Our
providers
are
able
to
see
the
child
in
their
own
space.
Our
physical
therapist
can
see
the
space,
the
families
don't
have
to
drive
even
15
or
30
minutes
and
as
well.
We
have
children
in
our
autism
clinic
that
are
more
comfortable
in
their
home
and
so
there's
a
totally
different
setup,
basically
for
them
when
they're
able
to
stay
in
their
home
and
see
the
physician,
so
the
telehealth
program
has
really
taken
off
next
slide.
H
H
H
They
go
through
a
didactic
program
and
they
as
well.
They
do
a
case
study,
so
basically
a
provider
like
say
a
family
practitioner
in
eastern
kentucky,
who
has
a
child
that
comes
in
with
autism.
They
are
empowered
to
treat
that
child
and
to
work
with
that
child
and
family
versus
having
them
on
a
waiting
list
for
a
referral
next
slide.
Please.
H
This
slide
shows
the
population
that
we
served
over
the
last
two
fiscal
years:
let's
go
year,
20
and
fiscal
year,
21
again
with
our
specialty
clinics,
our
audiology
therapy
services,
the
early
hearing,
detection
intervention
and
as
well
our
family
to
family
health
information
centers.
So
this
is
also
a
key
part,
not
only
the
care
coordination,
but
we
have
family
to
family
health
information
centers,
which
essentially
connects
one
family
to
another
family.
So
it's
almost
like
a
peer
support
system.
H
H
So
in
the
local
office
we
were
able
to
do
early
intervention
services
to
get
children
prepared
for
school
and
basically
ensuring
that
there
are
no
developmental
delays
and
if
there
are,
then
we
can
provide
services
to
counteract
that
next
slide.
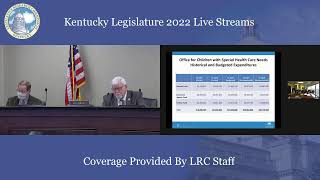
Please,
and
so
this
shows
our
budget,
our
historical
and
our
our
current
and
recommended
so
from
fiscal
year,
20
to
21
through
2024,
so
all
of
the
services
that
we
just
mentioned
the
some.
H
C
First
of
all,
I
just
want
to
say
kudos
for
your
echo
program.
I
think
that's
much
needed
and
it
sounds
like
it's
wonderful.
I
also
applaud
the
telehealth
services,
but
as
a
former
physical
therapist,
I
would
just
caution
physical
therapy.
They
actually
need
to
see
people
because
you
can
get
contractures
and
things
like
that.
So
I
don't
know
that
telehealth
is
great
for
that
over
the
long
term.
I
understand
the
need
for
the
pandemic,
but
I
guess
I
would
caution
about
that.