►
From YouTube: Budget Review Subcommittee on Human Resources (7-7-21)
Description
No description was provided for this meeting.
If this is YOUR meeting, an easy way to fix this is to add a description to your video, wherever mtngs.io found it (probably YouTube).
A
B
A
President
of
the
room
before
we
proceed
with
the
formal
agenda,
just
a
personal
point
of
order
here,
I'd
like
to
acknowledge
the
passing
of
senator
tom
buford
yesterday,
I'm
sure
most
folks
are
aware
of
that,
and
tom
certainly
was
a
valuable
member
of
our
caucus
and
he'll
be
sorely
missed
and
if
you
would
I'd
actually
join
with
me
in
a
moment
of
silence,
remembering
his
family
and
carol
his
wife
and
children,
stephanie
moe
and
their
grandchildren.
So
if
you
would
please
bail
with
me.
A
A
Before
we
begin
with
the
presentations
for
members
participating
remotely,
please
remember
to
meet
your
microphones
and
this
morning
we're
going
to
get
updates
on
funding
for
social
workers
in
the
department
of
community-based
services
for
commissioner
miranda
straub
and
her
staff,
and
this
issue
has
been
part
of
the
budget
discussions
in
the
past.
So
it's
kind
of
like
deja
vu
all
over
again.
So,
commissioner
and
other
presenters
are
here,
please
come
forward
and
identify
yourself
with
the
record.
E
Good
morning,
thank
you
so
much
senator
I'm
mara
miranda
straub.
Thank
you
all
for
the
invitation
for
our
staff
to
present
to
you.
Thank
you
for
caring
about
our
child
welfare
workers
and
the
children
and
youth
in
our
community.
We
have
a
presentation
prepared
for
you
that,
hopefully,
will
give
you
the
com,
the
understanding
of
where
we
are
and
where
we
want
to
go
and
where
we're
going
to
need
your
support.
Lisa
dennis,
who
is
our
deputy
commissioner,
will
be
presenting
the
first
part
of
this
presentation.
A
Appreciate
that
and
we're
going
to
keep
this
very
structured
today,
because
we
have
a
lot
of
committee
meetings
going
on
and
we're
going
to
try
to
conclude
this
by
11
30,
so
I'm
allocating
30
minutes
to
each
of
these
presentations
plus
questions.
So
members,
if
you
would
please
hold
your
questions
and
to
out
their
presentations,
I
think
that'll
help
us
go
a
little
bit
smoother.
So,
ladies
again,
if
you
didn't
find
yourself,
the
record
feel
free
to
feel
free
to.
A
F
Good
morning
again,
my
name
is
lisa
dennis,
and
I
am
the
deputy
commissioner
with
the
department
for
community-based
services.
Again,
we
want
to
say
thank
you
for
the
opportunity
to
be
with
you
today
and
present
on
the
department's
staffing
challenges
and
discuss
what
is
needed
to
be
able
to
build
capacity
to
serve
the
citizens
of
the
commonwealth.
F
From
approximately
a
year
ago,
kentucky
was
an
early
implementer
of
the
federal
legislation
known
as
family
first
prevention
services
act,
which
allows
public
child
welfare
agencies
for
the
first
time
to
access
federal
funding
for
prevention,
in-home
services.
This
was
funding
that
was
traditionally
utilized
for
foster
care,
guardianship
and
adoption
assistance.
F
One
of
the
anticipated
outcomes
with
the
shift
in
funding
and
practice
was
to
see
a
decrease
in
the
number
of
children
out
of
home
care,
as
kentucky
continues
to
invest
in
prevention
services.
We
anticipate
to
see
this
downward
trend
continue
and
more
children
and
families
serve
within
their
communities
with
in-home
services.
F
As
you
can
see
from
the
slide,
our
our
agency
received
right
at
114
000
intakes
during
the
calendar
year
of
2020,
and
if
you
will
look
at
the
third
column,
you
will
see
that
right
at
90.
000
of
those
intakes
involve
allegations
of
child
abuse
and
neglect,
and
the
fourth
column
shows
that
of
those
approximately
90
000
intakes
involving
allegations
of
child
abuse
and
neglect
that
right
at
45,
000
were
accepted,
that
which
means
they
met.
F
Acceptance
criteria
and
our
staff
responded
and
made
contact
with
families
and
completed
an
assessment,
and
then,
from
that
45
000.
Approximately
the
last
two
columns
shows
the
number
of
referrals
that
resulted
in
the
finding
either
substantiation
or
services
needed
the
the
last
column
just
breaks
that
apart
and
shows
the
number
of
substantiated
referrals
as
a
loan.
F
The
department
is
focused
on
it.
Excuse
me
again
in
addition
to
assessing
for
safety
and
risk,
which
is
what
our
staff
does
with
every
interaction
with
families
and
children.
They
are
also
focused
on
placement,
stability
and
the
best
placement
possible,
and
when
we're
talking
about
the
best
placement
possible,
it's
more
than
just
a
home
for
a
child,
it's
looking
for
a
home
or
a
placement
for
a
child
that
best
meets
their
identified.
Treatment
needs.
F
This
slide
looks
at
our
average
cps
caseload
caseloads.
We
know
that
case
loads.
Are
we
look?
We
can
look
at
case
loads,
a
variety
of
different
ways,
but
the
column
that
most
accurately
represents
the
experience
of
our
front
line.
Caseload
carrying
social
workers
is
the
last
column,
the
purple
column.
That
column
includes
all
of
our
current
cases.
It
includes
any
past
due
case
assignments,
and
then
we
divide
those
total
case
loads
case
counts
by
the
number
of
staff
that
we
have
available
to
carry
to
carry
a
case
at
any.
Given
time.
F
The
department
has
a
number
of
staff
that
we
can
we
consider
as
not
at
full
capacity.
These
are
staff
that
are
not
available
to
carry
a
caseload.
They
are
new
staff
that
are
in
training.
They
are
staff
that
are
on
extended
medical
leave.
They
may
be
on
desk
duty,
et
cetera,
so
to
be
to
give
a
accurate
reflection
of
what
caseloads
look
like
and
are
experienced
by
our
staff.
We
remove
those
staff
from
the
calculation
to
get
our
average
currently.
F
I
would
also
note
here
with
k
with
regards
to
caseloads.
This
is
a
statewide
average,
so,
depending
on
what
area
of
the
state
that
a
worker
is
located
in
their
experience
could
look
different.
For
example,
the
average
case
load
in
jefferson
is
closer
to
jefferson
is
closer
to
40.
They
it's
around
approximately
30
campbell,
county
and
davis
county
again
are
around
29
30.
so
again,
depending
on
where
staff
are
located,
their
experience
could
look
different.
F
This
is
the
statewide
average
and
I
wouldn't
know
just
one
other
thing
with
regards
to
case
low
numbers
when
looking
at
caseloads,
we
need
to
keep
in
mind
the
complexity
of
the
cases,
because
each
case
looks
different.
Currently,
workers
are
managing
all
types
of
cases,
low
or
lower
risk
cases,
as
well
as
high
risk
and
very
complex
cases,
as
well
as
in
home
out
of
home
care.
So
again,
each
case
looks
different.
It
has
to
be
considered
with
regards
to
its
needs
and
complexity.
F
This
this
slide
looks
at
turnover
within
dcbs
for
2020..
The
first
column
identifies
the
dcvs
department
overall,
as
well
as
each
of
the
nine
surface
regions,
and
then
we
have
two
columns.
One
is
with
internal
transfers
and
then
one
is
without
internal
transfers
by
the
accounted
by
the
personnel
cabinet
are
seen
as
a
positive
change,
which
is
a
positive
change
for
a
local
team
or
a
county,
but
for
the
department.
F
Overall,
it
doesn't
really
change
our
staffing
numbers
if
a
worker
moves
from
anderson
county
to
to
bullitt
county,
so
the
last
column
is
a
more
accurate
account
of
turnover,
and
the
other
thing
I
would
note
here
with
regards
to
turnover
is
this-
is
this
is
all
positions,
so
this
is.
This
is
everything
this
is
your
front
line
caseload
carrying
social
workers.
This
is
your
front
line
non-caselo
carrying
social
workers.
It
is
your
support
staff,
secretarial
staff,
your
supervisors,
regional
management,
et
cetera.
This
is
all
all
staff
in
each
of
these.
F
The
other
thing
would
note
with
regards
to
turnover
is
the
tenure
of
our
staff.
Our
workforce
is
a
very
young
workforce
at
this
point.
Currently
44
of
our
dcbs
caseload
carrying
and
social
workers
are
in
the
job
classification
of
the
social
services
worker,
one,
which
is
the
entry
level
position
to
qualify
for
a
social
service
worker.
In
one
position
you
have
to
have
a
social
work
degree
or
a
degree
in
a
related
field,
and
no
experience
is
required.
F
F
The
top
four
systemic
issues
identified
as
part
of
the
review
process
related
to
related
to
the
staffing
demands
and
experience
levels
of
staff,
caseload
demands,
management
of
different
levels
of
complexity
of
cases
and
retention
of
staff
and
being
able
to
fill
vacancies
timely
and
just
as
of
as
of
a
note
here,
there
was
218
cases
reviewed,
but
some
of
them
had
more
than
one
identified
systemic
issue.
So
if
you
total
the
columns
across
the
bottom,
it
will
be
greater
than
218.
E
E
When
that
happens,
our
capacity
is
lowered
to
provide
the
services
that
our
families
need.
We
have
a
difficult
time
retaining
employees
and
we
have
a
high
turnover
actually,
the
national
statistics,
without
institutional
support
or
care
for
advocates
or
child
welfare
workers
working
with
directly
with
trauma
on
the
front
line,
is
about
18
months
and
we're
right
there.
E
So
our
turnover
is
high.
That
creates
a
problem
of
capacity
for
us
and
for
our
families,
trauma
the
experience
of
trauma
and
secondary
trauma.
The
first
trigger
for
that
worker
is
the
desire
to
leave
work
work
to
flight
from
the
situation
next,
so
we've
implemented
a
safety
model,
and
this
is
a
practice
used
in
child
welfare
is
best
practice
to
assist
as
a
tool
to
assist
the
worker
and
in
making
decisions
about
the
safety
and
risk
at
multiple
points
in
the
case,
not
just
when
we
receive
the
case
or
when
there's
a
critical
incident.
E
So
this
a
tool
to
help
our
workers
make
decisions
so
that
that
is
a
new
model
that
we
have
instituted
next,
we
think
that,
yes,
the
council
is
right,
15
to
18
caseload
cases
per
worker
when,
with
the
severity
of
the
clients
that
we
see
is
accurate.
However,
the
severity
of
those
cases
vary
and
when
our
workers
are
inexperienced,
that
creates
a
problem.
So
what
we
want
to
do
is
create
an
alternative
response
to
be
able
to
go
from
traditional
investigation.
E
I'm
not
going
to
read
to
you,
but
look
at
the
traditional
investigation
tool,
an
alternative
response,
so
non-incident-based
an
assessment
of
the
strengths,
as
well
as
the
formal
determination
of
whether
mild
treatment
occurred
or
not,
and
the
different
with
that
a
differential
assignment
of
cases.
So
it's
not
only
the
amount
needs
to
be
reduced.
Therefore,
the
need
for
more
workers,
but
the
severity
of
the
cases
need
to
decide
how
many
cases
folks
can
take.
E
So
we
would
like
to
have
the
less
experienced
workers
have
the
less
traumatic
severe
cases
and
then
hire
clinical
experts
on
complex
trauma
to
be
able
to
have
smaller
caseloads
with
the
most
traumatized
families,
children
and
youth,
and
to
act
as
content
experts
for
the
younger,
less
experienced
workers.
Next.
E
So
here
are
the
phases
that
vcbs
has
engaged
in.
Since
I
became
commissioner
on
july
1st
phase
one
we
developed
a
stabilization,
we
turn
on
a
dime
like
all
of
you
during
covet.
What
do
we
need
to
do
to
stabilize
what
work
that
we
want
to
keep?
What
didn't
work
that
we
need
to
stop
doing?
Then
we
just
finished
doing
our
phase
two,
which
is
an
18-month
strategic
plan
that
deals
with
the.
How
are
we
going
to
design
services
with
a
lift
client
experience
in
mind?
E
How
are
we
going
to
decrease
barriers
and
increase
access,
and
then
that
will
be
evaluated
over
the
next
year
and
then
all
of
that
will
be
integrated
into
what
we're
calling
our
21st
century
three-year
strategic
plan.
It
is
important
to
note
that
in
this
process
we
have
recruited
our
own
existing
alumni,
families
and
youth,
as
well
as
front
line
and
every
level
25
members
of
dcbs
representing
every
level
and
every
region.
E
The
second
is
trauma,
resilience
and
engaged
healings.
This
is
the
secondary
drama
piece
for
our
own
staff
being
and
then
the
the
trauma
that
our
clients
experience.
So
we
begin
with
us
building
capacity,
strength,
support
organizational
policy
and
process
for
our
staff
and
then
being
able
to
do
drama
informed
care
with
all
of
our
children
and
youth.
So,
instead
of
what
did
you
do,
that
is:
what's
happened
to
you,
so
it's
a
more
collaborative
and
engaged
conversation.
E
Our
third
pillar
is
families,
children
and
youth,
all
families
from
bio
families,
to
foster
families
to
effective
king
king
and
the
fourth
is
health
and
wellness.
So
we're
looking
at
behavioral
health,
mental
health
and
the
opioid
crisis,
and
the
fifth
one
is
really
that
systemic
and
structural
piece
that
we
are
redesigning
as
a
backbone
for
dcvs.
E
How
do
we
implement?
How
do
we
evaluate,
and
how
do
we
create
systemic
and
structural
changes?
So
we
we
don't
keep
putting
a
band-aid
on
the
heart
attack,
for
example,
turnover
next
and
I'm
sorry,
I'm
speaking
fast,
not
only
because
I'm
cuban,
but
because
I
know
we
have
limited
time
so
we
want
to
our
vision
is
to
build
a
robot's,
virtual
and
in-person
workforce.
E
On
july
11th,
we
began
to
add
a
lot
more
in-person
meetings,
accessibility
to
all
of
our
clients
across
the
state,
as
well
as
we're
looking
at
reinforcing
what
we
learned
from
covid,
which
is
that
folks,
our
folks
really
do
a
great
job.
We
actually
served
70
000
more
people
in
snap.
We
answer
calls
in
three
to
seven
minutes
as
opposed
to
30..
E
Error
rate
has
decreased,
so
we
have
lots
of
benefits
that
we've
learned
a
robust
virtual
workforce
and
an
in-person
workforce
is
really
what
would
work
best
for
us,
and
now
we
implemented
that
on
july
11th,
and
we
will
continue
to
evaluate
our
goal,
is
to
continue
to
reduce
brick
and
mortar,
since
a
certain
percentage
over
staff
can
do
their
work,
virtually
or
staff
can
rotate.
So,
for
example,
if
I
just
had
a
critical
incident
had
a
gun
to
my
head,
I
had
to
remove
a
child
with
cigarette
burns
on
their
back,
etc.
E
So
we
have
open
concept
desk
where
folks
can
come
in
plug
in
their
laptop,
make
copies,
speak
with
a
supervisor
and
go
back
and
see
families
in
their
own
home
or
go
back
to
their
office
at
home,
we're
working
on
a
work-life
balance.
You
know
how
important
that
is
so
lots
of
flexibility
and
then
moving
into
revise
and
modernize
all
the
physical
physical
components
of
the
cvs
and
become
a
living
example
of
who
we
are
as
an
agency
and
what
we
do
and
what
we
value
next.
E
So
budget
requests.
I
just
want
to
give
you
an
update
in
2022,
we
requested
from
the
governor
and
the
governor
recommended
a
structural
piece
for
us,
which
is
the
internal
infrastructure,
around
training,
supervision,
secondary
trauma,
debriefing
groups
etc,
as
well
as
adding
50
to
70
additional
social
workers.
That
will
be
those
highly
skilled,
clinical
social
workers
that
can
support
our
young
staff
to
while
they
have
cases
and
be
able
to
have
the
more
complex
cases
for
those
who
are
more
clinically
have
the
clinical
expertise
to
manage
that.
E
So
we're
finalizing
a
plan
for
the
20
million
dollars
that
was
awarded
to
us
for
prevention,
and
we
have
krista
bell
here
who
can
answer
our
primary
and
secondary
prevention.
We
will
come
back
to
you
during
the
session
and
ask
for
designing
a
division
of
primary
and
secondary
reporting
directly
to
the
commissioner's
office,
because
we
need
to
stop
just
having
family
when
they
have
exhausted
their
resources
and
are
in
dire
crisis.
E
We
need
to
patch
folks
upstream
so
we're
moving
towards
a
primary
and
secondary,
we'll
always
do
tertiary
where
er
triage
take
care
of
who
comes
in
bleeding.
However,
we
need
to
get
ahead
of
the
curve
and
begin
to
do
a
primary
and
secondary
intervention.
We've
been
very
successful,
with
family
first
and
with
sky,
doing
the
secondary
and
primary
information,
so
we're
finalizing
that
plan
on
a
child
welfare
prevention
plan
as
well
as
we
we're
in
the
process
of
developing
our
2023
budget
request.
E
A
Thank
you
appreciate
the
presentation
that
is
very
concise
and
to
the
point.
Probably
this
agenda
could
be
entitled
deja
vu
all
over
again,
because
I
think
the
three
groups
that
are
presenting
today
also
presented
two
years
ago
when
formulating
the
budget.
So
here
we
are
again
and
we
will
open
for
questions
and
if
you
don't
mind
I'll
start
with
on
your
slide
number
three.
F
Again,
I
think
that
relates
we
implemented
family
first
prevention,
service
prevention,
services,
act
and
part
of
that
plan,
and
implementation
was
looking
at
how
to
provide
services
in
home
and
to
reduce
those
out
of
home
care
numbers,
and
we
think
the
department
really.
The
department
thinks
that
the
implementation
of
fellaini
first
has
has
led
to
our
decrease
in
number
of
children
out
of
home
care.
A
A
A
G
Sure
I'd
be
happy
to
answer
that.
I
mean
chris
bell:
I'm
an
executive
advisor
with
the
dcbs
commissioner's
office
with
the
implementation
of
the
family.
First
prevention
services
act.
It
has
allowed
us
for
the
first
time
ever
to
draw
down
federal
dollars
or
federal
reimbursement
at
a
50
percent
rate
for
those
prevention
services
that
we
know
are
successful
in
keeping
children
safely
at
home
with
their
families.
G
So
we
think
that
there
were
not
impacts
of
the
pandemic
in
in
what
we
saw
there,
and
so
we,
you
know,
think
that
our
expanded
prevention
services
have
been
success,
successful
and
will
continue
to
be
successful.
So
those
evidence-based
practices
under
family
first
are
how
we
are
preventing
children
coming
into
care,
preventing
future
maltreatment
and
really
leveraging
that
to
move
upstream
to
primary
and
secondary
prevention,
so
providing
services
to
families
even
before
abuse
and
neglect
can
occur.
G
Sure
so
we
have
the
data,
as
I
said,
prior
to
implementation
of
family.
First,
our
funding
for
prevention
services
for
those
intensive
in-home
services
to
families
was
very
limited.
We
had
waiting
lists
even
though
the
services
that
we
that
we
were
able
to
provide
through
those
contracts
were
very
successful
between
93
and
96.
G
They
were
very
limited
and
in
most
parts
of
the
state
we
had
waiting
lists
for
those
services.
So
when
we
were
able
to
leverage
additional
federal
funding
beginning
in
october
of
2019,
we
were
able
to
expand
those
contracts
for
services
and
serve
more
families,
reducing
our
waiting
list,
and
so
what
our
fiscal
management
reports
indicate
is
that,
with
that
additional
six
million
dollar
investment
in
prevention
and
state
fiscal
year
2020?
What
we
realized
was
a
15
million
dollar
reduction
in
out
of
home
care
costs.
G
We're
able
to
keep
children
out
of
more
expensive
congregate
care
or
residential
settings,
and
so
by
really
focusing
those
services
on
the
front
end
to
keep
children
at
home
with
their
families
and
to
keep
children
in
family-based
settings
even
when
they
do
have
to
come
into
care.
We're
really
able
to
see
that
return
on
investment
in
terms
of
cost,
but
we're
also,
I
think
what
is
even
more
important,
is
to
prevent
children
from
having
to
experience
the
trauma
of
being
separated
from
their
families
or
having
to
enter
the
foster
care
system
at
all.
E
E
So
we're
really
looking
at
what
they
need
and
how
we
can
provide
that
in
community
as
opposed
to
in
residential
care-
and
I
don't
know
if
christa
mentioned,
but
we
had
a
96
reduction
in
residential
care
of
the
youth
that
participated
in
the
family
first.
So
all
of
our
residential
partners
are
looking
at
intensive,
comprehensive
wraparound
services
to
have
been
alternative
to
residential.
We
will
always
need
residential
for
some
children,
but
not
for
the
many,
as
we
have
had,
we've
been
on
a
downward
trend,
and
we
want
to
continue
to
do
that.
A
G
No
sir,
it
is
not
included
in
that
9122
children,
the
waiting
lists
are
for
and
that
we've
experienced
in
the
past
were
for
family
and
president
preservation
services,
and
so
referrals
are
made
to
that
program
for
children
who
are
at
imminent
risk
of
removal.
So
without
those
intensive
in-home
services
we
are
not
able
to
mitigate
the
risk
factors
that
would
that
would
require
them
to
come
into
care.
G
So
when
we
have
waiting
lists
sometimes
and
we
can't
access
resources
or
access
immediate
intensive
services,
sometimes
the
only
alternative
in
the
past
was
to
bring
children
into
out
of
home
care.
So
potentially
of
that
9100
there
there
could
be
children
reflected
in
that
number
that
came
into
care
while
they
were
waiting
less
in
that
area
of
the
state,
but
with
the
additional
investment
of
prevention
dollars
and
the
ability
to
also
leverage
federal
funding.
Now
for
prevention,
we
have
been
able
to
eliminate
the
vast
majority
of
those
waiting
lists.
A
E
Share
your
concern,
that's
why
we
want
to
build
the
infrastructure
and
bring
the
content
expertise
that
is
needed
for
this
young
workforce.
In
addition,
we're
really
looking
at
measuring
child
abuse
against
ourselves
so
that
we
can
look
at
our
own
progress
as
we
go
forth
and
we'll
be
able
to
do
a
presentation
on
that
to
you.
E
A
And
I
agree
with
that,
but
my
concern
is
the
footprint
of
government
keeps
getting
bigger
and
bigger,
and
if
we're
not
really
making
an
impact
on
the
the
number
of
lives
that
we're
impacting
them,
we
haven't
been
successful.
So
I
would
look
forward
to
that
continued
conversation
and
to
see
some
specific
measures,
keeping.
E
E
I
Been
in
in
this
field
for
several
several
years,
I
have
such
a
great
passion
for
it.
I
do
have
a
question
about
what
is
the
average
age
of
your
frontline
social
worker.
You
may
not
have
that
information,
but
if
you
could,
let
us
know
that
down
the
road.
That
would
be
very
helpful.
You
know,
of
course,
the
younger.
They
are
the
greater
impact
emotionally,
it
has
on
them,
and
I
don't
know
if
there
have
been
any
long-term
studies
on
their
mental
and
physical
health.
E
Senator
westrom,
we
also
measure
what
we're
measuring
is
the
amount
of
experience
and
the
majority
of
our
staff
right
now
is
have
less
than
one
year
40.
But
now
these
are
complex
cases
that
me,
as
a
clinical
person,
who've
done
with
trauma
would
not
carry
more
than
12
or
15.
It's
a
folks
without
experience
carrying
pretty
damaging
traumatic
experiences
with
our
clients.
So
that
is
a
concern,
and
we
thank
you
for
your
understanding
of
that,
and
I
do
not
know
that,
but
we
will
get
that
information.
I
I
J
F
I
G
I
G
So
we
utilize
a
number
of
evidence-based
practices
that
each
have
their
own
timeline.
They
are
tailored
for
different
ages
of
children,
but
the
maximum
length
of
time
without
an
additional
approval
is
12
months
that
is
established
by
the
federal
federal
law
under
family
first,
so
beyond
12
months.
It
requires
that
that
family,
that
you
go
through
the
documentation
again
to
establish
that
that
child
as
a
candidate
for
foster
care.
G
I
I
I
A
Representative
westrom,
we
still
have
three
people
on
thecube.
Please
note
the
time
we're
almost
a
quarter
till
we're
going
to
adjourn
by
11
30,
we'll
be
a
little
bit
challenged,
but
I
have
in
the
queue
representative,
moser
center
berg
and
then
representative
prenty,
then
we'll
move
on
the
next
presentation.
So
representative
moser,
please
feel
free.
K
You've
been
very
busy
doing
great
work,
and
I
I
do
appreciate
all
that
you
have
focused
on
in
terms
of
staffing
and
kind
of
updating
the
the
five
pillars
of
how
to
how
to
keep
kids
from
out
of
home
placement.
I
know
that
there
are
some
pilots.
I
think
that
that's
what
you
were
referencing
was.
Is
this
the
multi-systemic
therapy
pilots
that
you're
talking
about,
and
can
you
just
talk
briefly
about
what
those
are
and
in
terms
of
the
really
targeted
treatment
and
efficient
use
of
resources
for
families.
E
Thank
you.
Thank
you,
senator
moser,
and
thank
you
for
your
support
for
that.
What
this
yes
is
multi-systemic
family
therapy,
which
is
expensive,
but
that
means
that
there
is
a
team
of
experts,
content
experts
that
work
with
that
family.
They
have
a
very
slow
caseload,
very
low
case
load.
They
will
work
with
a
family
directly
they're
in
the
community,
no
less
than
an
hour
from
where
the
family
and
client
lives.
E
Therefore,
if
a
child
or
a
youth
at
three
o'clock
on
a
friday
night
wants
to
run
away
from
home,
okay
came
home,
intoxicated
or
whatever
that
that
family
can
actually
call
and
that
worker
can
have
a
session
with
that
family
right
then,
and
there
on
the
weekend,
etc.
It
has
proven
incredible
successful
in
other
states,
there's
been
a
pilot
in
jefferson
county
by
home
of
the
innocents
who
has
really
shown
incredible
outcomes
for
the
children
that
would
end
up
dead
in
a
gang
or
in
juvenile
justice.
E
That's
targeted
to
those
really
difficult
kids,
who
have
a
lot
of
issues
and
a
lot
of
trauma
and
has
been
very
successful.
Now
we're
looking
at
doing
a
pilot
in
northern
kentucky,
as
well
as
in
the
bluegrass
region.
We
also
do
functional
family
therapy,
which
is
another
in
community,
wrap
around
comprehensive
services.
K
F
K
E
F
K
E
Yeah
you're
right
those
conversations
have
been
had
from
day,
one
that
I
got
here.
They
were
half
they
were
have
before
I
got
here,
but
very
intentionally
since
I
got
here
and
what
we're
working
with
them
is.
What
else
can
you
provide
that
we
need,
for
example,
sexually
reactive
youth.
We're
always
gonna
need
residential
help
for
that.
We
we
so
they're.
Looking
at
those
and
they're
also
looking
into
moving.
E
For
example,
the
children's
home
of
northern
kentucky
and
home
of
the
innocents
are
two
beautiful
examples
of
residential
getting
out
reducing
residential
and
it
into
multi-systemic
therapy
with
us.
So
this
is
a
joint
collaboration,
a
conversation
we
told
them.
This
is
going
to
be
a
three
to
four
year
process
start
looking
at
your
budget
start
looking
reframing
at
intensive
community
based
services
models
and
that's
how
we're
ended
up
where
we
are
today,
they're
very
much
part
of
the
conversation
and
I'm
bored
in
regards
to
moving
into
community
services
and
reducing
residential
care.
E
K
C
C
C
Relative
to
children
who
aren't
in
state
custody
because
to
me
that
would
be.
You
know
one
marker
of
long-term
success
that
these
children
are
getting
educated
and
being
able
being
put
in
a
position
where
they're
going
to
be
able
to
to
take
care
of
themselves
as
adults.
Do
we
keep
track
of
that
at
all.
G
We
we
do
track
outcomes
and
those
types
of
measures
for
youth
who
leave
foster
care
at
18
or
if
they
extend
commitment
and
we
care
after
age
18..
So
there
are
a
number
of
things
that
we
keep
track
of
for
those
youth,
including
high
school
or
ged,
completion,
the
rate
of
attendance
of
college,
whether
they
have
health
care,
whether
they
are
able
to
obtain
and
maintain
employment
and
and
other
outcomes
for
those
youth.
D
You,
mr
chair,
I
want
to
clarify,
did
you
say
family
first
started
october
19?
Is
that
when
it
was
first
implemented?
Okay,
I
just
want
to
clarify
that.
I
commend
you
for
your
vision.
Thank
you
for
your
work.
I
think
the
vision
of
flexibility
is
good,
but
the
question
has
to
do
with
slide
two,
that
you're
responsible
for
delivering
services
and
reduce
poverty.
How
do
you,
how
does
dcbs
reduce
poverty.
G
So
those
are
some
of
the
ways
that
we
work
to
address
poverty,
specifically
with
regard
to
our
child
welfare
prevention
services,
though,
in
addition
to
those
evidence-based
practices
that
we've
talked
about
that
are
specifically
geared
to
addressing
issues
such
as
mental
health,
substance
use
and
in-home
parenting
skills.
There
are
also
flex
funds
included
in
those
contracts
for
prevention,
services,
so
say,
for
example,
that
transportation
is
a
major
challenge
for
a
family
to
be
able
to
obtain
and
maintain
gainful
employment.
G
There
are
flex
funds
that
are
available
for
use
for
those
families,
for
that
with
whom
we
are
working
in
home
to
assist
with
perhaps
a
car
repair
or
utilities,
or
other
things
that
are
perhaps
a
challenge
with
keeping
the
children
safely
at
home.
So
that
is
one
of
the
ways
that
we
help
to
address:
address
challenges
associated
with
poverty,
with
the
families
that
we
are
working
with
on
the
child
welfare
side
as
well.
D
Thank
you
I
just
I.
I
did
home
health
physical
therapy
for
10
years,
and
I
saw
real
quick
that
we
were
handing
out
a
lot
of
fish,
not
teach
people
how
to
fish,
and
I
feel
like
it
needs
to
be
collaborative
between
the
legislature
and
the
cabinet
to
reduce
poverty.
I
think
that
what
you're
talking
about
using
flex
funds
for
transportation,
to
keep
somebody
in
a
job
is
an
empowering
thing
and
that's
good,
that's
good.
I
think
we
need
policies
too.
I
think
public
assistance
reform
is
important
to
try
to
encourage
people.
D
You
know
that
can
be
in
the
workforce
and
we
need
to
get
people
to
work
and
as
far
as
raising
social
workers
salaries,
you
know.
If
we
get
more
people,
less
people
receiving
and
more
people
paying
into
the
tax
base,
then
we
can
increase
salaries
and
maybe
have
a
decreased
need
for
social
workers,
because
there
won't
be
so
many
in
the
system.
But
those
those
are
just
my
comments.
But
thank
you
for
your
work
and
thank
you
for
your
answer.
I
think
that's
good,
but
do
whatever
you
can
to
empower
people.
Thank
you.
A
A
A
If
the
commissioner
of
the
presenters
are
here,
please
identify
yourself
for
the
record
and
feel
free
to
proceed,
and
I
encourage
members
again
hold
your
questions
to
the
end
of
the
presentation,
but
certainly
be
cognizant
of
the
time
we've
got
about.
30
minutes
left
two
presentations
left.
Thank
you.
J
J
For
the
department
for
aging
and
independent
living,
our
mission
is
simply
to
promote
the
welfare,
dignity
and
independence
of
older
adults
and
individuals
with
physical
disabilities
and
adults
in
need
of
a
guardian.
We
are
one
of
the
newer
departments
if
you
will,
but
I
always
say
we
are
the
department
that
you
don't
know
you
need
until
you
have
a
family
loved
one
or
friend,
who
is
truly
in
need
of
services,
as
you
can
see
here,
the
the
programs
in
oversight
that
we
provide,
we
oversee
the
older
americans
act,
programs,
which
are
your
senior
centers.
J
J
We
also
have
the
newly
created
office
for
dementia
services
that
was
passed
in
this
previous
session
that
will
be
housed
within
the
department
in
addition
to,
and
what
I'm
here
to
talk
to
you
today
about
which
is
state
guardianship,
so
just
an
overview
for
those
of
you
who
are
not
familiar
with
state
guardianship.
State
guardianship
is
a
program
for
individuals,
age,
18
or
older.
They
support
individuals
who
have
a
cognitive
impairment
that
prevents
their
ability
to
make
informed
decisions.
J
J
There
is
no
decision
on
behalf
of
the
department
for
us
to
determine
who
can
or
cannot
come
in.
We
have
to
simply
follow
the
different
district
court
rules
and
appointments
that
assign
individuals
to
us.
So
what
rights
do
the
individuals
have
when
they
come
into
state
guardianship
and
what
rights
do
they
not
have?
J
This
is
an
overview.
There
are
a
lot
of
things
that
out
in
the
general
community
state
guardianship
that
they
think
state
guardianship
can
do.
However,
by
law.
There
are
things
that
we
cannot
do.
State
guardianship
cannot
force
treatment,
medications
or
control
an
individual's
behavior.
We
cannot
lock
up
or
restrain
individuals.
J
We
cannot
keep
a
violent
perpetrator
from
harming
another
person
or
force
providers
to
serve
an
individual.
We
cannot
create
resources
or
benefits
for
individuals
and,
despite
what
some
individuals
may
think,
state
guardianship
is
not
a
funding
agency
for
individuals.
We
only
have
what
benefits
and
finances
that
that
individual
has
available
to
them.
There
is
no
secret
plot
of
fund
that
state
guardianship.
Has
these
individuals
have
the
same
access
to
resources
that
you
and
I
have
available.
J
So,
within
state
guardianship
there
are
four
different
levels:
you,
an
individual
may
be
under
full
guardian,
full
conservator,
meaning
that
our
staff
are
responsible
for
both
the
personal
and
financial
affairs
of
the
individual.
An
individual
may
be
under
only
personal
guardianship,
meaning
that
we
only
oversee
their
personal
affairs.
J
They
may
be
there
for
a
conservator
and
responsible
for
only
financial
affairs.
I
know
in
the
media.
Conservatorship
has
gotten
a
lot
of
attention
with,
what's
been
going
on,
so
just
to
bring
you
aware
to
that.
There
are
also
limited
guardian
and
limited
conservator,
meaning
a
judge
has
made
the
decision
that
state
guardianship
needs
to
step
in
only
within
specific
areas
of
interest
to
that
individual
to
keep
them
safe.
J
So,
as
we
alluded
to
earlier
in,
I
know
for
many
of
you,
who've
been
here
for
quite
some
time.
There
have
been
multiple
presentations
done
on
state
guardianship
and
over
the
past
10
years,
11
years
we
have
presented
on
cases
that
have
continuously
gone
up
because
of
covid.
For
the
first
time
in
state
guardianship
history,
our
cases
have
decreased
courts
were
not
open
to
open.
Generally,
they
were
only
open
for
emergency
guardianship,
appointments
and
for
bench
trials
from
march
20th
of
2020
to
may
1st
of
2021.
J
So
one
of
the
things
I
want
you
all
to
look
into
as
we
are
moving
forward
is
the
number
of
active
clients
we
have
had
and
then
the
green
line
as
you'll
note
are
the
number
of
deceased
clients
that
we
have
in
the
red
line
is
the
number
of
resigned
clients.
A
resigned
client
is
an
individual
in
which
they
either
have
their
rights
reinstated
by
a
court
or
a
family
member
or
friend,
has
stepped
in
and
proven
to
the
courts
that
they
are
able
to
make
decisions
on
their
behalf.
J
You
will
notice
for
2020,
there
were
564
deaths,
which
is
almost
100
more
than
the
previous
year,
and
this
was
in
fact
due
to
covid,
specifically
covid
19,
truly
impacted
state
guardianship.
You
can
see
here
that
24
of
our
population
tested
positive
for
covid
and
4
passed
away.
These
are
180
individuals
who
lost
their
life
too
soon
to
covet
the
majority
of
which
did
live
in
long-term
care,
but
also
want
to
recognize
the
significant
impact
that
this
has
played
on
staff.
J
As
many
of
these
individuals,
our
guardianship
staff
knew
for
a
long
time
or
for
a
short
time,
but
just
want
to
bring
you
all
to
bring
this
to
your
attention
so
through
the
pandemic
and
as
we
are
still
currently
going
through
that
we
have
truly
implemented
multiple
areas
of
support
for
staff.
We
have
partnered,
with
the
community
crisis
response
board
to
ensure
that
everyone
is
aware
of
the
needs
that
are
out
there
and
what
to
do
and
they
find
themselves
in
crisis
for
our
staff.
J
J
We
have
done
multiple
trauma-informed
care
trainings
on
the
impact
of
anxiety,
depression,
post-traumatic
stress
due
to
covid.
We
are
promoting
flexibility
and
secondary
and
tertiary
trauma.
I
know
commissioner
straub
presented
on
that
some
earlier.
We
have
also
provided
self-care
and
leadership
trainings
for
many
of
you
all,
as
as
you
all
are
our
leaders.
We
know
that
as
leaders
we
have
to
demonstrate
self-care
for
others
to
see
that
it
is
okay.
It
is
okay
to
take
time
off
to
take
care
of
yourself.
J
This
is
coordinated
on
behalf
of
the
department
for
behavioral
health,
developmental
intellectual
disabilities
and
we
are
encouraging
all
of
our
guardianship
staff
to
attend
and
just
oh,
we
can
go
back
one
and
just
to
be
clear.
When
we
talk
about
guardianship
staff,
we
talk
a
lot
about
the
field
staff,
the
staff
we
have
out
in
the
field,
but
we
also
have
staff
who
are
processing
benefits
and
on
the
fiduciary
side
of
the
house,
and
some
of
our
fiduciary
benefits
staff
they're,
not
in
the
field,
but
they
have
tertiary
trauma.
J
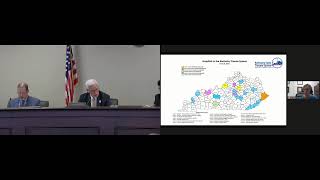
J
So
what
does
this
look
like?
What
does
guardianship
look
like
across
the
state?
These
are
the
number
of
current
cases
broken
up
by
our
guardianship
region.
This
map
is
a
little
different
than
what
the
dcbs
map
is,
but
this
gives
you
an
idea
as
to
how
many
cases
are
in
each
region.
These
regions
are
designed
based
upon
the
number
of
current
guardianship
cases,
and
there
is
time
to
time
in
which
the
regions
may
adapt,
as
court
cases
may
may
evan
flow
and
you'll
notice.
J
The
most
is
in
the
metro
region,
louisville
and
surrounding
counties
with
1200.
and
all
in
all,
there
are
over
400
cases.
So
where
are
our
state
guardianship
individuals?
They
are
in
each
of
your
all's
communities.
They
are
all
across
the
state,
the
majority
of
which
are
between
waiver
residential,
including
the
scl
supports
for
community
living
waiver
and
the
acquired
brain
injury
waiver,
as
well
as
in
long-term
care,
including
icfs,
skilled
nursing
and
personal
care
homes.
We
have
some
individuals
who
are
currently
residing
out
in
the
community.
J
They
are
living
active
lives
out
in
the
community
and
each
of
these
levels
of
care
are
based
on
the
least
restrictive
environment,
with
the
funds
that
each
individual
has
available
to
them.
Again,
we
have
no
extra
pot
of
money
for
anyone
to
go
to.
This
is
the
same
resources
that
you
and
I
have
to
make
decisions
for
our
loved
ones
as
we're
moving
forward.
As
we
had
alluded
to
earlier,
the
courts
are
opening
back
up.
We
are
starting
to
see
our
new
appointments
increase.
J
You
can
notice
that
they
almost
double
from
january
to
may.
We
anticipate
at
the
time
this
presentation
was
submitted.
We
were
at
the
end
of
june,
so
we
did
not
have
those
numbers,
but
we
anticipate
that
june's
numbers
will
have
increased
as
well.
So
what
does
I
mean?
What
is
the
impact
on
staff
with
the
number
of
cases
that
are
increasing
across
the
state,
so
you
will
see
that
we
did
add
10
new
staff
in
from
2018
to
2019.
There
was
a
small
increase
within
our
guardianship
budget.
J
However,
we
have
seen
a
decrease
in
staff
turnover
now.
Personally,
I'd
like
to
say
it's
because
I
came
on
as
commissioner
two
weeks
before
the
pandemic
and
that
that's
why.
However,
we
recognize
that
during
the
pandemic,
there
were
not
a
lot
of
individuals
who
were
moving
in
between
jobs
during
the
pandemic.
J
We
have
worked
really
hard
to
support
our
staff
through
this
and
we
are
working
even
harder
to
bring
on
more
staff
as
we'll
discuss
later
so
for
the
4
400
guardianship,
individuals
that
have
no
one
else
to
make
decisions
for
them
again.
State
guardianship
is
there.
We
have
103
that
are
out
in
the
field
and
32
that
work
in
frankfurt
to
process
benefits
and
fiduciary
responsibilities.
J
Due
to
time,
I
will
not
go
through
and
read
each
of
these,
but
just
want
to
note
that
we
do
have
checks
and
balances.
Our
field
staff
cannot
invent
complete
inventory
and
issues
checks.
We
are
field
staff,
complete
inventory
and
then
contact
our
fiduciary
staff,
who
then
process
checks.
We
have
complete
and
separate
alignment
of
our
programs
to
ensure
there
is
not
any
ill
will
being
done
with
regard
to
our
guardianship,
individuals
in
the
management
of
their
finances
and
their
their
benefits.
J
So
one
of
the
things
I
am
really
excited
to
share
with
you
all
today.
I
know
many
times.
Commissioners
have
come
before
you
and
said
we
need
help.
We
need
help,
we
need
help.
We
looked
within
our
own
cabinet
and
we
found
some
help.
We
truly
believe
that,
with
secretary
freelander
partnerships
make
progress,
and
in
december
of
2020,
the
department
of
aging
and
independent
living
signed
a
contract
with
dms
to
draw
down
a
50,
50
federal
match.
We
looked
within
our
own
data
and
saw
that
96
of
our
4
400
individuals
received
medicaid
and
recognized.
J
We
could,
on
behalf
of
the
work
our
guardianship
workers
were
doing,
draw
down
a
50-50
match,
so
we
can
receive
up
to
5.7
million
dollars
in
additional
funds
because
of
the
individuals
that
we're
serving
who
are
on
medicaid
because
of
this
drawdown.
It
creates
64
new
guardianship
positions,
the
majority
and
field
and
some
in
the
benefits
and
fiduciary
sides
of
the
house.
J
So
if
you
look
at
the
three
colors
on
here,
the
blue
line
is
the
current
case
load
and
when
we
say
caseload,
this
means
the
number
of
field
staff,
number
of
benefits,
staff
and
fiduciary
staff
who
are
currently
working
in
combination
together
to
support
our
individuals,
and
this
is
broken
out
by
regions
with
the
map
that
I
had
shown
to
you
previously
and
so
you'll
look
to
see
kind
of
where
those
numbers
were.
The
green
is
the
anticipated
result
of
when
we
hire
on
the
64
additional
staff,
where
those
case
loads
will
go.
J
J
J
in
order
to
bring
us
to
our
the
national
recommended
caseload
standards,
we're
looking
at
needing
another
45
additional
staff
members
to
get
us
there
to
get
us,
and
we
have
worked
really
really
hard
to
get
to
that
point.
The
next
few
slides-
and
I
won't
go
over
these-
you
can
read
over
these.
It's
just
the
focus
on
what
we
are
doing
internally.
We
are
truly
working
on
modernizing
guardianship.
For
so
long
it
has
been
keep
your
head
down.
J
Keep
your
self
out
of
court,
keep
your
client
out
of
court,
but
we
have
truly
implemented
in
working
on
modernizing
our
state
guardianship
system.
We
are
providing
a
multitude
of
guardianship
staff
training
which
have
not
been
done
before,
as
well
as
we
have
our
first
ever
guardianship
strategic
plan
and
those
goals
are
listed
on
the
final
slide.
Thank
you
very
much
senator
meredith
and
thank
you
to
each
of
the
committee
members
for
listening
today.
H
More
yeah
they
are
court
appointed.
They
have
to
petition
and
file
an
application
for
appointment
as
the
guardian
and
conservator,
and
it
is
up
to
the
judge
to
determine
if
they
qualify.
Each
court
has
a
different
way
that
they
determine
whether
that
individual
is
appropriate
or
not.
Some
courts
do
courtnet
search.
Do
some
background
checks.
Ask
some
questions.
Others
do
not,
but
it's
up
to
that
individual
judge.
A
H
J
And
the
one
thing
that
I
will
add
to
that
is
our
state
guardianship.
Individuals
are
sorry
our
state
guardianship
workers,
those
cases
are
assigned
based
upon
their
current
caseload
and
what
their
expertise
is
all
of
our
state.
Guardianship
workers
all
have
to
meet
standard
background
checks
and
criteria
to
move
forward.
J
A
J
L
Thank
you
senator
my
name
is
dick
bartlett.
I
am
the
emergency
preparedness
and
trump
wax
and
the
trauma
coordinator
now
for
the
kentucky
hospital
association
and
its
foundation.
The
kentucky
hospital
research
and
education
foundation,
and
I
believe,
on
the
zoom
link,
is
dr
julia
costas,
who
is
the
chairman
of
our
kentucky
trauma,
advisory
committee
and
she's?
Also
the
associate
director
for
the
university
of
kentucky's
kentucky
injury
prevention
and
research
center
at
the
university
of
kentucky.
A
B
L
But
the
trauma
that
we're
dealing
with
this
system
actually
was
created
in
2008
with
the
support
of
dr
bill
hacker.
Who
was
our
commissioner
at
the
time
in
order
to
create
a
system
to
deal
with
saving
lives
and
as
a
result,
as
we
can
save
lives
or
mitigate
the
damage?
That's
done
by
an
damage
to
the
body
by
an
accident
or
an
injury
of
some
sort.
You
know
it
does
save
economic
lives
because
we
keep
return
people
to
productive
society
again.
L
So
there's
a
direct
relationship,
but
the
law
did
create
a
system.
It
did
create
recognized,
trauma,
centers
and
it
tried
to
create
a
comprehensive
trauma
care
program
that
would
be
established
by
the
department
of
public
health.
Dr
hacker
basically
said
to
us:
you
know
mr
bartlett
nancy
galvani
mike
rusty
was
our
president
at
the
time.
I
will
birth
the
baby,
but
you
guys
have
got
to
raise
it,
because
what
we
got
was
a
trauma
system
without
any
money,
and
it
talks
about
in
the
slide
here
to
the
extent
that
funds
are
available.
L
L
So
what
essentially
happened
was
that
the
cabinet,
through
a
contract,
that
we
had
at
kentucky
hospital
association
and
our
research
and
education
foundation,
included
the
trauma
care
system
support,
and
I
became
not
only
the
emergency
preparedness
coordinator
for
the
program,
but
I
also,
as
another
duty
assigned
became
the
state
trauma
coordinator,
so
I
fulfilled
that
trauma
director's
position
that
you
saw
in
the
previous
slide.
It
also
created
a
trauma
advisory
committee.
18
members
serve
without
compensation,
they
are
appointed
by
either
the
governor
or
by
the
secretary,
and
they
serve
without
compensation.
L
It
could
be
reimbursed
for
travel
and
related
expenses,
but
we
have
not
had
that
many
physical
meetings,
because
we
have
no
budget
for
that.
So
we've
been
meeting
virtually
almost
since
the
beginning,
using
the
assets
and
resources
of
the
cabinet
for
health
and
family
services,
it
did
establish
a
fund
and
the
fund
was
originally
intended
to
hold
those
dollars
which
were
created
either
by
the
activities
of
the
program
or
by
any
state
funds
and
by
other
monies
that
were
generated
well,
we
we
were
fortunate
in
that
we
did
have
some
monies
donated
to
the
program.
L
The
good
samaritan
foundation
foundation
from
the
methodist
conference
here
in
kentucky
donated
some
monies,
which
we
were
able
to
apply
to
various
activities.
The
foundation
for
healthy
kentucky
donated
some
monies.
We
had
a
initial
grant
from
mesa,
which
was
an
er
physicians
group
which
got
our
state
trauma
registry
signed
up
and
funded,
but
we
did
not
use
this
fund
for
that
purpose.
L
Unfortunately,
the
history
of
the
panel
here
is
that
you
in
the
history
tended
to
go
and
raid
these
kinds
of
funds
for
balancing
the
general
fund,
and
so
we
felt
that
it
might
not
be
a
good
idea
to
use
some
of
these
opportunities
here
through
this
account.
So
we
did
it
through
the
kentucky
hospital
research
and
education
foundation,
which
is
a
501c3.
L
We
were
able
to
give
the
organizations
involved
the
appropriate
tax,
letters
and
credits
that
they
needed
and
in
the
in
the
case
of
a
bequest
that
we
got
for
about
a
quarter
million
dollars.
It
allowed
the
foundation
to
actually
invest
those
funds
while
preserving
the
capital,
and
we
have
a
substantial
amount
of
interest
that
we're
using
now
to
plow
back
into
the
program
for
educational
support
and
activities.
So
it's
been
a
very
good
symbiotic
relationship.
L
It
was
established
by
kiprick
using
funds
from
mesa,
and
it
is
currently
supported
by
funds
from
the
national
highway
traffic
safety
administration
on
a
grant,
so
it
is
grant
supported.
We
started
out
with
only
three
trauma:
centers
in
the
state
university
of
louisville
university
of
kentucky
and
kosair
children's
hospital.
We
are
now
up
to
21
across
the
state
and,
as
dr
hacker
has
said,
on
several
situations
and
I'm
not
sure
what
we're
going
to
do
here.
L
Let
me
go
back
here
and
click
on
this
one,
this
map,
if
it'll
come
up,
let's
see
here,
I'm
not
sure
what
I
did
ben,
but
I'm
going
to
see
if
this
will
help
bring
it
up.
Well,
I'm
going
to
try
one
more
time
there
we
go.
This
map
shows
our
current
layout
and
it
also
shows
that
we
have
a
couple
of
facilities
that
are
in
development.
L
So,
in
addition
to
the
21,
I've
got
a
facility
down
in
warren
county.
That's
working
on
a
level
three
which
is
a
in
between.
We
go
one,
two
three
and
four
level.
One
and
two
are
usually
academic,
related
medical
teaching
facilities
or
having
residents
in
the
facility
level.
Three
has
many
of
those
kinds
of
skills
and
capabilities,
in-house
24
hours
a
day
or
available
immediately
on
call
and
a
level.
L
4
is
a
well-developed
community
emergency
department
with
dedicated
assets
and
resources,
and
it's
it's
a
step
up
and
above
and
beyond
what
you
would
consider
a
normal
emergency
department,
so
we've
got
21,
we've
got
about
three
or
four
that
are
in
development,
and
I
think
this
is
an
amazing
progress
that
we've
been
able
to
make.
Considering
that
we've
got
a
system
that
does
not
have
any
funds
to
support
it.
The
process
is
that
facilities
have
to
be
verified.
L
There
are
standards
that
we
have
to
follow
for
the
level
one
two
and
three
facilities.
Those
standards
are
set
by
the
american
college
of
surgeons
committee
on
trauma
and
they
actually
come
in
and
do
a
verification
every
three
years
of
those
facilities.
It's
a
very
intense
and
expensive
proposition.
L
We
did
our
level
four.
We
developed
our
own
criteria.
We
actually
modeled
it
after
some
general
guidance
from
the
american
college,
plus
some
good
examples.
We
got
from
tennessee
ohio,
minnesota
and
other
states
to
create
a
document
which
gave
us
a
good
set
of
verification
criteria
which
is
built
into
our
regulations
now
and
it's
defined
in
there.
So
it's
it's
clear
and
we
go
in
and
we
will
verify
those
folks.
L
The
designation
becomes
kind
of
important,
sometimes
for
third-party
payers.
They
require
you
to
be
part
of
a
designated
system.
If
you're
going
to
use
the
billing
profiles
that
go
along
with
being
a
trauma
system,
we
also
have
been
very
fortunate
that
once
we
have
a
designated
trauma
facility,
our
partners
at
the
kentucky
cabinet
for
transportation
have
gone
back
and
where
you've
got
the
h
sign,
that's
on
the
highways
near
a
trauma
center.
They
have
gone
back
and
added
our
request
at
no
charge
to
this
to
our
program.
L
I'm
just
trying
to
make
a
designation
differentiation
as
to
what
we've
done
to
try
to
let
the
public
know
that
this
is
a
trauma
center,
as
opposed
to
other
hospitals
that
might
be
in
the
area.
We
also
developed
a
comprehensive
trauma
program,
resource
manual,
built
heavily
upon
our
partners
in
minnesota
and
tennessee,
and
it
becomes
a
very
good
guide
for
these
folks.
So
they've
got
some
instructions
and
information
and
models
and
samples
of
what
forms
and
things
should
look
like
and
how
they
should
operate
in
their
facility.
L
So
we
do
have
the
fund.
The
fund
that
we've
got
is
actually
today
running
a
balance
of
about
thirty
eight
thousand,
eight
hundred
and
sixty
dollars.
Where
did
those
funds
come
from?
They
came
from
those
designation
and
verification
fees.
We
do
pay
our
verification
team
a
thousand
dollars
per
day.
Sometimes
we
can
get
more
than
one
verification
done,
but
that's
where
those
verification
fees
are
used
and
they
also
cover
any
of
our
other
costs
related
to
the
operation
of
the
basic
program.
L
Right
now,
in
our
contract
at
kha,
through
khraf,
we
have
about
15
000
a
year
in
there,
which
is
used
specifically
targeted
for
paying
for
the
fees
of
our
site,
verification
team
because
of
the
pandemic.
We've
only
done
one.
This
last
year,
I've
got,
though,
probably
anywhere,
between
six
and
seven
coming
up
in
this
fiscal
year,
which
just
started
so
it's
going
to
be
a
busy
year
and
we
will
use
all
of
our
allocated
funds
and
probably
some
from
the
last
allocation.
L
So
that's
how
we've
been
able
to
handle
that
there
have
been
a
few
classes
and
courses
that
I,
as
a
trauma
coordinator,
have
gone
to,
and
we
also
draw
those
out
of
those
funds.
The
question
may
become
all
right,
you're
the
trauma
coordinator.
Where
do
you
get
paid
from?
I
do
not
get
paid
from
this
fund.
L
I
am
a
contractor
at
this
point.
I
stepped
back
as
full-time
trauma,
emergency
preparedness
coordinator
and
went
on
a
part-time
basis,
so
I'm
doing
trauma
and
I'm
doing
some
relationships
with
some
of
our
federal
partners,
but
I
am
paid
through
the
grant
that
we've
got
in
the
contract
that
we've
got
through
the
cabinet,
because
there's
a
direct
relationship
between
trauma
and
emergency
preparedness
and
being
prepared
for
a
mass
casualty
event
and
things
of
that
nature.
L
So
the
salary
that
I
get,
which
is
very
small
about
10
hours
a
week,
is
what
I'm
currently
compensated
for
to
deal
with.
Trauma
comes
from
that
contract.
We
are
not
taking
any
funds
from
this.
The
concern
at
this
point,
which
is
why
I've
got
the
last
slide
up
here,
is
that
you
know
I
am
74
just
turned
74
on
the
29th,
and
you
know
if
I
were
to
step
away
and
step
back.
There
is
no
state
employee.
There
is
no
contrary
to
what
it
said
in
the
earlier
slide.
L
We
have
talked
about
having
a
state
director
and
a
straight
registrar
and
so
forth.
There
are
no
state
employees
in
this
program.
We've
got
to
create
a
stable,
permanent
foundation
at
some
point
for
this
trauma
program.
We've
looked
at
this
and
we've
talked
about
this
during
previous
administrations,
but
it
has
just
not
been
received
at
this
point,
so
I
think
that's
important
that
we
bring
this
forward.
We
need
to
talk
about
the
registry
software,
dr
kasich,
and
her
team
are
supported
again
by
the
grant
from
the
national
highway
traffic
safety
administration.
L
It
points
primarily
to
the
kentucky
hospital
association,
where
I
have
trauma
pages
on
the
kha
kyh.com
site,
we'd
like
to
have
some
support
for
meetings,
educational
programs.
Our
regulations
require
a
rural
trauma.
Team
development
course
for
new
trauma
centers
and
for
the
medical
directors
of
existing
trauma
centers
to
keep
them
up
to
speed
and
keep
their
skills
up.
Advanced
life
support,
advance,
burn
life,
support
and
things
of
that
nature.
Burns
are
considered
part
of
trauma.
L
We
currently
have
only
one
burn
center
in
the
state
of
kentucky
one:
the
university
of
louisville
hospital,
the
burn
center
that
was
part
of
the
university
of
kentucky
basically
stepped
back.
They
will
take
burns
up
to
about
10
percent
in
their
medical
icu
unit.
They
cook
the
norton's
burn
center
will
do
the
same
with
burned
children
up
to
that
point
they
get
transferred
out.
They
will
either
go
to
the
university
of
louisville
now
or
they
will
go
south
to
vanderbilt
or
north
to
cincinnati
and
shriners
hospital
or
over
east
towards
kabul.
L
So
you
know
we
we
we're
trying
to
develop
an
additional
burn
life,
support
training
for
hospitals
to
be
able
to
support
and
take
care
of
severely
burned
patients
until
we
can
work
out
arrangements
for
their
longer
term
care.
To
that
extent,
we
also
are
doing
educational
programs.
This
fall
using
our
bequest
monies,
we're
going
to
do
an
advanced
burn
life
support
and
a
rural
trauma
team
course
for
hospitals
at
eastern
kentucky.
L
The
abls
course
is
designed
to
provide
the
basic
skills
for
hospitals
in
small
rural
community
access
and
and
regional
hospitals
to
be
able
to
to
care
for,
stabilize
and
prepare
for
transfer
for
the
most
serious
patients
out
and
the
rural
trauma.
Team
development
course
is
there
to
help
develop
new
trauma
centers
and
we're
going
to
replicate
that
working
with
our
health
care
coalition
in
eastern
kentucky,
I'm
talking
with
their
coordinator
about
doing
a
similar
program
in
the
eastern
part
of
the
state.
Probably
late
fall
early
winter.
L
So
we
can
develop
additional
programs
for
eastern
kentucky
to
help
build
the
trauma
system
in
that
part
of
the
state.
We'd
like
to
go
ahead
and
try
to
get
the
full-time
equivalent
of
a
trauma,
program,
manager,
training,
coordinator
to
kind
of
coordinate
and
manage
this
program.
It
is
right
now
doing
through
kha.
We
would
be
more
than
willing
to
continue
that
relationship
with
the
state.
We've
been
good
partners
with
them.
A
That's
that's
worrisome
and
again.
I
appreciate
the
detailed
explanation
on
the
ask,
but
I
think
what's
missing
from
this
discussion
is:
what's
the
real
impact
of
this
I
mean
this.
This
has
been
in
place
since
2008
and
never
has
been
funded
other
than
the
funding
sources
you
have
mentioned
and
we've
survived,
and
why
do
we
want
to
commit
the
money
to
this?
If
it's
it's.
L
L
13
650,
actually
it's
more
than
that,
and
we
are
still
getting
some
of
this-
that
the
pandemic
has
caused
some
of
the
registrars
to
be
a
little
slow
in
getting
their
data
in
there.
I
expect
that
number
will
be
several
thousand
more
so
at
least
13
000
500,
kentucky
residents
have
been
impacted
by
this
trauma.
System
have
have
been
in
our
trauma.
Centers
have
been
seen
and
stabilized
by
the
physicians
and
the
trauma
teams
that
are
out
there.
You
know
in
a
trauma
center,
even
even
a
level
four
trauma
center,
an
emergency
department.
L
L
What
is
wrong
right
now?
What
can
we
do
to
stabilize
that
patient
and
create
the
best
outcome
possible?
It's
really
a
sight
to
behold
when
you
see
what
one
of
these
teams
looks
like
and
what
they're,
what
they're
really
involved
with
in
terms
of
trying
to
help
engage
that
patient
and
we've
tried
to
make
a
decision.
L
That's
an
awful
lot
of
information
that
they've
got
to
process
and
assemble
x-rays
and
scans
that
they've
got
to
get
together
tests
that
they've
got
to
run
and
if
they
make
that
decision
that
it's
got
to
go
then
that
next
process
starts
we've
got
to
get
that
ambulance
crew
back
in
we've
got
to
make
sure
that
patient
is
packaged
and
ready.
We've
got
to
make
rel
connections
with
a
level.
You
know
three
two
or
one
facility
down
the
line.
L
If
it's
really
bad,
it
may
have
to
be
flown,
which
may
mean
we
may
have
to
scramble
an
aircraft
to
come
in
and
pick
up
that
patient
and
package
it
and
fly
it
to
a
distant
level,
one
or
level
two
trauma
center
or
a
burn
center.
So
there's
an
awful
lot
that
goes
on.
That
makes
a
difference
and,
like
I
said,
over
13
000
people
were
impacted
in
2020
and
that's
the
preliminary
numbers.
That's
not
the
final
number.
A
And
I
think
that's
what's
missing
from
the
presentation,
jameson
barton,
it's
not
a
criticism
of
you.
We
want
to
give
you
a
limited
amount
of
time
to
do
this,
but
you
know
that
13
000.
That
is
an
impression
sizable
number.
I'm
would
be
curious
about
the
cost
associated
with
that
13
000
is
because
what
I'm
looking
for
is
how
we
can
impact
this
to
truly
save
the
commonwealth
and
in
our
citizens.
B
A
D
A
Need
to
educate,
I
think,
our
legislator
as
to
why
this
is
important
for
kentucky.
It's
a
matter
of
coincidence,
a
good
friend
of
mine
stopped
by
my
community
last
friday,
who
happened
to
grow
up
in
litchfield
kentucky.
He
worked
at
my
hospital
as
a
restaurant.
Therapist
became
a
trauma.
Surgeon
is
now
head
of
the
trauma
center
in
georgia.
The
network.
L
A
L
Program
is
outstanding
and
we've
looked
at
several
ways.
In
order
to
fund
a
trauma
system,
I
will
tell
you
that
the
distracted
driving
law,
which
the
general
assembly
passed
a
number
of
years
ago,
the
original
proposal
for
the
fees
coming
from
the
distracted
driver
law,
were
targeted
at
supporting
our
trauma
care
system.
But
you
know
at
the
time
the
general
assembly
chose
to
you
know
we
need
to
do
that
for
balancing
the
budget
in
other
areas,
so
that
would
move.
A
L
Knowing
that
we
had
a
short
period
of
time-
and
there
was
a
second
ask
of
of
us
and
kiprick-
we
are
also
scheduled
to
appear
on
july,
the
21st
at
three
before
the
medicaid
oversight
and
advisory
committee
and
dr
kostisch
is
working
on
some
specific
powerpoints
and
data
presentations
for
that
committee.
To
talk
more
about
the
fiscal
impact
and
the
potential
savings
and
relationship
of
the
trauma
system
to
the
medicaid
costs
and
so
forth.
So
there's
be
more
of
that.
I
think
coming
in
the
next
presentation.
A
A
C
Very
much
first
of
all,
I
want
to
say
thank
you
for
this
presentation.
I
am
to
me
this
is
extremely
personal,
because
I
have
worked
in
a
level
one
trauma
center.
You
know
over
the
last
40
years,
so
I'm
on
the
receiving
end
of
everybody
who
comes
into
the
state,
and
I
also
am
very
aware
aware
of
the
of
the
importance
of
the
data
in
the
trauma
registry.
C
L
C
M
Or
patience
and
trauma
system
facilities
we
can
make
those
estimates.
We've
never
actually
tried,
because
it
would
take
many
hours
and
a
lot
of
computer
resources
and
we
don't
have
a
budget
for
them,
but
we
can
certainly
have
a
shot
at
it
for
the
state
as
a
whole.
We
look
at
statewide
injury
data
that
are
available
in
the
state
hospital
discharge
data
system,
with
which
I'm
sure
some
of
you
are
familiar.
A
But
you
know,
I
would
think,
though,
that
our
mco
partners
could
provide
us
with
some
information.
With
that
regard,
I
mean
since
they're
processing
the
claims
and
they
have
to
voted
appropriately.
Then
they
could
probably
make
a
reasonable
estimate
for
us,
but
we'll
attempt
to
do
that,
but
we
need
to
truly
try
to
identify
that
the
best
that
we
possibly
can.
B
Yes,
sir,
thank
you,
mr
chairman,
when
I
was
looking
at
this
map
at
first,
I
thought
well
eastern
kentucky's
kind
of
covered
with
schedule
four,
but
then
I
realized
like
up
in
greenville,
where
I'm
from
you
have
trauma
in
kabul
and
saint
mary's.
So
do
they
get
kentucky?
Patients
is
that
in
your
statistics
of
the
sixteen
thousand
or
thirteen
thousand
no.
M
L
We
do
have
situations
where
burned,
for
example,
are
going
to
cobble
huntington
from
that
that
area
out.
There,
though,
some
are
transferred
by
helicopter
towards
the
university
of
louisville,
vanderbilt
and
north
towards
cincinnati.
A
lot
of
the
children
have
been
going
north
to
shriners
in
cincinnati,
which
has
now
moved
over
towards
dayton.
Yeah.
B
L
Burn
beds
are
very
expensive
to
sustain,
and
so
that's
you
know
that's
why
so
many
of
these
burn
centers
are
beginning
to
shut
down
they
it's
just
very
expensive.
I
I
really
take
my
hat
off
to
dr
smith
and
the
team
at
the
university
of
louisville
who
who
chose
to
go
in
the
opposite
direction.
He
just
he
wanted
to
do.
He
wanted
to
take
and
make
a
difference
when
he
became
chief
medical
officer
down
there.
He
and
I
spent
some
time
talking
about
that
and
they
expanded
and
grew
that
program
and
I've
I'm
encouraging
them.
L
There
are
very
few
burn
beds
in
the
state
and
that's
why
we're
also
promoting
advanced
burn
life,
support
programs
to
help
the
small,
rural
and
regional
hospitals
to
increase
their
ability
to
take
care
of
these
people
until
if
they
are
really
bad,
we
can
find
a
bed
and
that
bed
may
be
in
another
state.
It
could
be
north
carolina,
ohio.
We
don't
know.
A
A
Part
of
this
before
we
adjourn
just
reminded
our
next
committee
meeting,
will
be
august
4th
and
for
members
who
want
to
participate
remotely
you'll
be
provided
with
a
zoom
link,
as
well
as
downloading
the
information
for
that
meeting,
and
is
there
any
other
business
to
come
before
this
committee?
If
not
entertain
a
motion
to
adjourn
motion
in
a
second,
we
stand
a
germ.
Thank
you
for
your
time
appreciate
all
right.